
Septic Mucormycosis in Acute T-Cell Leukemia: A Case of Lichtheimia Corymbifera Detection
This report discusses a case involving a 43-year-old patient with acute T-cell leukemia who developed septic symptoms and unique targetoid bluish skin lesions after chemotherapy. Despite initial negative blood cultures, histopathological analysis revealed Lichtheimia corymbifera as the causative pathogen, illustrating the aggressive nature of mucormycosis. The patient experienced multiple tissue infarctions and ultimately succumbed to the infection. This case highlights the challenges in detecting mucormycosis and the critical need for rapid identification and treatment.

Septic Mucormycosis in Acute T-Cell Leukemia: A Case of Lichtheimia Corymbifera Detection
E N D
Presentation Transcript
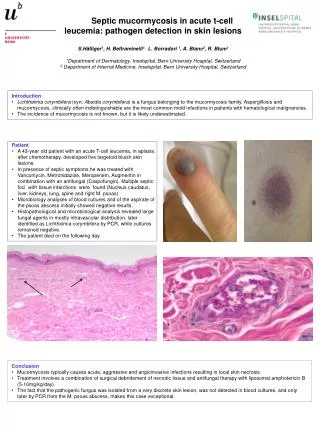
Septicmucormycosis in acute t-cellleucemia: pathogendetection in skin lesions S.Häfliger1, H. Beltraminelli1, L. Borradori 1, A. Blanc2, R. Blum1 1Department of Dermatology, Inselspital, Bern University Hospital, Switzerland 2 Department of Internal Medicine, Inselspital, Bern University Hospital, Switzerland • Introduction • Lichtheimiacorymbifera(syn. Absidiacorymbifera) is a fungus belonging to the mucormycosisfamily. Aspergillosis and mucormycosis, clinically often indistinguishable are the most common mold infections in patients with hematological malignancies. • The incidence of mucormycosis is not known, but it is likely underestimated. • Patient • A 43-year old patient with an acute T-cell leucemia, in aplasia after chemotherapy, developed five targetoid bluish skin lesions. • In presence of septic symptoms he was treated with Vancomycin, Metronidazole, Meropenem, Augmentin in combination with an antifungal (Caspofungin). Multiple septic foci with tissue infarctions were found (Nucleus caudatus, liver, kidneys, lung, spine and right M. psoas). • Microbiology analyses of blood cultures and of the aspirate of the psoas abscess initially showed negative results. • Histopathological and microbiological analysis revealed large fungal agents in mostly intravascular distribution, later identified as Lichtheimiacorymbifera by PCR, while cultures remained negative. • The patient died on the following day. • Conclusion • Mucormycosis typically causes acute, aggressive and angioinvasiveinfections resulting in local skin necrosis. • Treatment involves a combination of surgical debridement of necrotic tissue and antifungal therapy with liposomal amphotericin B (5-10mg/kg/day). • The fact that the pathogenic fungus was isolated from a very discrete skin lesion, was not detected in blood cultures, and only later by PCR from the M. psoas abscess, makes this case exceptional.





