Download
1 / 18
180 likes | 390 Vues
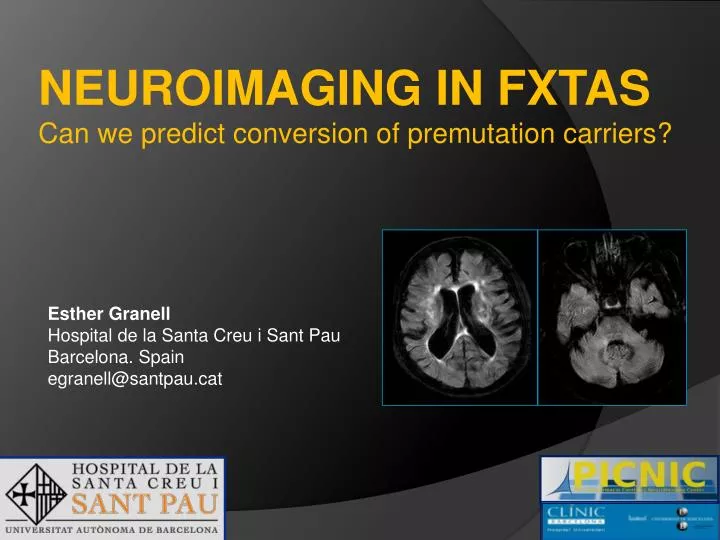
NEUROIMAGING IN FXTAS Can we predict conversion of premutation carriers?. Esther Granell Hospital de la Santa Creu i Sant Pau Barcelona. Spain egranell@santpau.cat. BACKGROUND.

E N D
NEUROIMAGING IN FXTAS Can we predict conversion of premutation carriers? Esther Granell Hospital de la Santa Creu i Sant Pau Barcelona. Spain egranell@santpau.cat
BACKGROUND Fragile-X-associated Tremor/Ataxia Syndrome (FXTAS) is a late onset neurodegenerative disorder occurrying in carriers of a premutation expansion (55 to 200 repeats) of the Fragile X Mental Retardation (FMR1) gene
BACKGROUND FMR1 gene RNAm translation FMR1protein NORMAL <54 CGG Fragile X Syndrome (FXS) FMR1 gene RNAm absent protein (methylation) (no transcription) FULL MUTACION >200 CGG Fragile X Tremor Ataxia Syndrome (FXTAS) FMR1 gene excess RNAm normal or low protein Toxic gain-of-function: inclusion formation and neurological dysfunction PREMUTATION 55-200 CGG
“Definitive” disease: 1 major radiological + 1major clinical “Probable”disease: 1 major radiological + 1minor or 2 major clinical “Possible disease”: 1 minor + 1 major radiological Diagnostic criteria • Major Radiological: WM, MCP and brainstem hyperintensities • Minor Radiological: brain, WM lesions moderate/severe brain atrophy • Major Clinical: intentional tremor, gait distubances • Minor Clinical: parkinsonism, loss of short memory executive disturbances Some FXTAS develop cognitive decline and eventually dementia, this having been mainly described in men. Up to date, it remains unknown which carriers will develop FXTAS and cognitive decline late in life
PURPOSE • To investigate if 3T MRI markers can differentiate FXTAS from non-FXTAS subjects, which may be potentially useful in predicting conversion of premutation carriers to FXTAS • To evaluate the relationship between MRI markers and cognitive-neuropsychological disturbances
METHODS Prospective, cross-sectionalstudy of 44 subjects (30 premutation carriers and 14 controls),aged 33-80, matched for age and sex • 3T (Philips Intera 2.1) MRI included3D FLAIR and 3D-T1 MPRAGE. Conventional, previouslydescribed MRI findingswere assessedbytwoexperiencedneuroradiologists • Neurological and neuropsychologicalevaluations:executive, memory, attention, global intelligence, and conductual • Cortical thickness (Freesurfer) and hippocampalvolume (FS) and hippocampalshape (SPHARM) wereanalyzed on 3D MPRAGE imagessearching for potential MR markers • Statisticalanalysisincludedgroup-comparisons (Student´st-test and one-way ANOVA) and a General Lineal Model
RESULTS MRI findings in FXTAS patients included: • Middle cerebellar peduncle, brainstem, and cerebral white matter hyperintensities • Cerebellar, brainstem and brain atrophy
RESULTS 1b 1c 1a 11 patients fulfilled FXTAS-criteria (women and men), 2 women having dementia: 2a 2b 2c These 2 women having FXTAS and dementia showed predominant frontal and temporal lobe atrophy, and white matter hyperintensities
RESULTS-Cortical thickness • There was selective decrease in cortical thickness in frontal and temporal regions, already present in the premutation state Young Pre-Young Control Elder Pre-Elder Control FXTAS-Elder Pre
RESULTS-Hippocampal volume and shape • Additionally, there were changes in hippocampal volume and its shape in the premutated and FXTAS state, more profound in those patients with dementia. Hippocampal volume in D FTXAS <non D FXTAS<Elder Pre (p=0.015 and 0.037) Young pre-Young control FXTAS-Elder pre D FXTAS-non D FXTAS
RESULTS-Neuropsychology On neuropsychology, therewasevidence of prefrontal and temporal impairment in premutatedpatientsalongthediseaseprocess • (FrBSe) Frontal System Behavior Scale: Apathy, dishinibition and executive disfunction in premutated patients: Premutatedvs Control (Total scale p= 0.021) FXTAS vs Elder pre (Apathy p=0.087) D FXTAS vs. Non-D FXTAS ( Apathy P=0.04) • Left hippocampal cognitive disturbances: AVLT (Auditory Verbal Learning Test) Immediate AVLT: FXTAS vsPremutated (p=0.042) Delayed AVLT: D FXTAS vs non-D FXTAS (p=0.074)
CONCLUSION • There are MRI changes already present in the premutated state in the frontal and temporal brain regions • These reflect impairment of related brain functions. 3T MRI may provide biomarkers, which could be clinically useful
REFERENCES I 1)Jacquemont, S, et al.Fragile X Premutation Tremor/AtaxiaSyndrome: Molecular, Clinical, and NeuroimagingCorrelates. Am. J. Hum. Genet. 72:869–878, 2003 2) Rodriguez-Revenga L, et al. Motor and mental dysfunction in mother-daughtertransmittedFXTAS. Neurology 2010 (in press) 3)A. Inagakia, A. Iidab, M. Matsubarac and H. Inagakid. Positron emission tomography and magnetic resonance imaging in spinocerebellar ataxia type 2: a study of symptomatic and asymptomatic individuals. European Journal of Neurology 2005, 12: 725–728 4)M.R.R. Gonçalves, L. P. Capelli, R. Nitrini, E. R. Barbosa, C. S. Porto, L. T. Lucato and A. M. Vianna-Morgante. Atypical clinical course of fxtas: rapidly progressive dementia as the major symptom. Neurology 2007;68;1864-1866 5)S. Jacquemont, R.J Hagerman, P.J Hagerman, M.A Leehey. Fragile-X syndrome and fragile X-associated tremor/ataxia syndrome: two faces of FMR1. Lancet Neurol 2007 Jan; 6 (1): 45-55
REFERENCES II 5)S. Jacquemont, R.J Hagerman, P.J Hagerman, M.A Leehey. Fragile-X syndrome and fragile X-associated tremor/ataxia syndrome: two faces of FMR1. Lancet Neurol 2007 Jan; 6 (1): 45-55 6) M. A. Leehey, E. Berry-Kravis, S. Min, D. A. Hall, C. D. Rice, L. Zhang, J. Grigsby, C. M. Greco, A.Reynolds, R. Lara, B J. Cogswell, S. Jacquemont, D.R. Hessl, F. Tassone, R. Hagerman. Progression of Tremor and Ataxia in Male Carriers of the FMR1 Premutation. Movement Disorders 2007; 22 (2): 203-206 7) M.A Leehey, R.P Munnhoz, A.E. Lang, J.A. Brunberg, J. Grigsby, C. Greco, S. Jacquemont, F. Tassone, A.M Lozano, P. Hagerman, RJ Hagerman. The Fragile X Premutation Presenting as Essential Tremor. Arch Neurol Vol 60, Jan 2003: 117-121 8)J. S. Adams, P. E. Adams, D. Nguyen, J. A. Brunberg, F. Tassone, W. Zhang, K. Koldewyn, S. M. Rivera, J. Grigsby, L. Zhang, C. DeCarli, P. J. Hagerman and R. J. Hagerman Volumetric brain changes in females with fragile X-associated tremor/ataxia syndrome (FXTAS) Neurology 2007;69;851-859
Acknowledgements • Collaborators: • O Lopez • G Llebaria • G Monté • G Sanchez • M Delfino • Y Vives • Genetics: • M Mila • L Rodriguez • A Sanchez • Neuroradiology: • B Gómez • J Ruscalleda • M De Juan • F Núñez • Patients and Controls • Hospital Clinic/IDIBAPS • H Santa Creu i Sant Pau • Neurology: • J Pagonabarraga • J Kulissevsky • E Muñoz • E Tolosa PIC, IFAE, UAB • MR technical staff FIS 07/770