Download
1 / 41
450 likes | 1.7k Vues
Munir Gharaibeh, MD, PhD, MHPE mgharaib@ju.edu.jo. Pharmacology of Autonomic Nervous System. Anatomic and neurotransmitter features of autonomic and somatic motor nerves. Anatomy of the Autonomic Nervous System. Sites of Origins Length of Preganglionic and Postganglionic neurons.

E N D
Munir Gharaibeh, MD, PhD, MHPE mgharaib@ju.edu.jo Pharmacology of Autonomic Nervous System
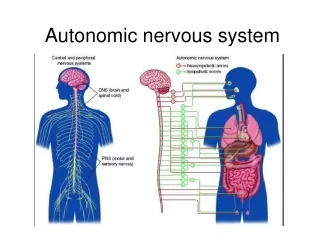
Anatomic and neurotransmitter features of autonomic and somatic motor nerves.
Anatomy of the Autonomic Nervous System • Sites of Origins • Length of Preganglionic and Postganglionic neurons. • Ratio of preganglionic: postganglionic
Direct Effects of Autonomic Nerve Activity on some Organs Systems. Drug effects are similar but not identical.
Direct Effects of Autonomic of Nerve Activity on some Organs Systems. Drug effects are similar but not identical.
Direct Effects of Autonomic Nerve Activity on some Organs Systems. Drug effects are similar but not identical.
Direct Effects of Autonomic Nerve Activity on some Organs Systems. Drug effects are similar but not identical.
Direct Effects of Autonomic Nerve Activity on some Organs Systems. Drug effects are similar but not identical
Direct Effects of Autonomic Nerve Activity on some Organs Systems. Drug effects are similar but not identical
Schematic illustration of a generalized cholinergic junction
Life Cycle of Acetylcholine • Choline is transported into the presynaptic nerve terminal by a sodium-dependent choline transporter (ChT). This transporter can be inhibited by hemicholinium drugs. • In the cytoplasm, acetylcholine is synthesized from choline and acetyl Co-A (AcCoA) by the enzyme cholineacetyltransferase (ChAT). • Acetylcholine is then transported into the storage vesicle by a second carrier, the vesicle-associated transporter (VAT), which can be inhibited by vesamicol. • Peptides (P), adenosine triphosphate (ATP), and proteoglycan are also stored in the vesicle.
Life Cycle of Acetylcholine • Release of transmitter occurs when voltage-sensitive calcium channels in the terminal membrane are opened, allowing an influx of calcium. The resulting increase in intracellular calcium causes fusion of vesicles with the surface membrane and exocytotic expulsion of acetylcholine and cotransmitters into the junctional cleft. This step can be blocked by botulinum toxin. • Acetylcholine's action is terminated by metabolism by the enzyme acetylcholinesterase. • Receptors on the presynaptic nerve ending modulate transmitter release.
Nicotinic transmission at the skeletal neuromuscular junction
Nicotinic transmission at the skeletal neuromuscular junction • ACh released from the motor nerve terminal interacts with subunits of the pentameric nicotinic receptor to open it, allowing Na+ influx to produce an excitatory postsynaptic potential (EPSP). • The EPSP depolarizes the muscle membrane, generating an action potential, and triggering contraction. Acetylcholinesterase (AChE) in the extracellular matrix hydrolyzes ACh.
Diagram of the intestinal wall and some of the circuitry of the enteric nervous system.
Diagram of the intestinal wall and some of the circuitry of the enteric nervous system (ENS). • The ENS receives input from both the sympathetic and the parasympathetic systems and sends afferent impulses to sympathetic ganglia and to the central nervous system. • Many transmitter or neuromodulator substances have been identified in the ENS. AC: absorptive cell CM: circular muscle layer EC: enterochromaffin cell EN: excitatory neuron EPAN: extrinsic primary afferent neuron IN: inhibitory neuron IPAN: intrinsic primary afferent neuron LM: longitudinal muscle layer MP: myenteric plexus NP: neuropeptides SC: secretory cell SMP: submucosal plexus
The major groups of cholinoceptor-activating drugs, receptors, and target tissues.
Cholinergic Agonists or Parasympathomimetcs • Definition: • Drugs which produce effects similar to those observed during the stimulation of postganglionic parasympathetic nerve fibers or have actions similar to acetylcholine.
Cholinergic Agonists or Parasympathomimetcs • Choline Esters. • Alkaloids. • Cholinesterase Inhibitors or Anticholinesterases.
Cholinergic Agonists or Parasympathomimetcs • Choline Esters: • Acetylcholine: • Naturally released ACh from the cholinergic nerve endings. • Very short acting because of rapid hydrolysis by AChase enzyme. • Used only in experimentation.
Methacholine: • Used in in the diagnosis of bronchial asthma ”Methacholine Challenge” • Carbachol: not used clinically because of nicotinic activity • Bethanechol: • Works mainly on M3( smooth muscles and glands), but weak at M2, so minimal cardiac effects. • Synthetic, long acting, used orally or s.c.. • Used in gastric and bladder atony, when there is no obstruction. • Causes flushing, sweating, colic.
Cholinergic Agonists or Parasympathomimetcs • Choline Esters. • Alkaloids: produce similar actions to ACH but inconsistent • Muscarine: present in some species of mushroom (Amanita muscaria), can cause poisoning. • Pilocarpine: • not hydrolyzed by cholinesterase • works mainly on M3 receptors. • used topically in glaucoma. • Nicotine
Nicotine • Uses:Non medical use( smoking and as an insecticide) and medical use in smoking cessation • Kinetics: • Rapidly absorbed through skin, lungs, and gut • For smoking cessation, used orally as a gum or topically as a patch. • Works on the ganglia, parasympathetic, sympathetic, motor end plate, CNS). • Dependence:due to activation of nicotinic receptors on neurons in the brain’s dopaminergic reward pathway(venrtal tegument area). • Nm stimulationcan lead to fasiculations, spasms, and depolarizing blockade. • Nn stimulation can lead to: • High heart rate • Vsoconstriction • High gastric motility and secretions. • Increased respiratory rate, due to chemoreceptor activation. • Medullary emetic chemoreceptor stimulation, so nausea and vomiting.
Varnicline(Chantix) • Partial nicotinic agonist. • Highly effective in supporting smoking cessation. • May be associated with psychiatric symptoms, including suicidal ideation.
Cholinergic Agonists or Parasympathomimetcs • Choline Esters. • Alkaloids. • Cholinesterase Inhibitors or Anticholinesterases: • Reversible • Alcohols: e.g. Edrophonium • Carbamic acid esters: e.g. Neostigmine, Carbaryl. • Irreversible( Organophosphates): e.g. Echothiophtae, Soman, Malathion
Cholinest Cholinesterase Inhibitors or Anticholinesterases erase Inhibitors or Anticholinesterases • Mechanism of Action: • Inhibit cholinesterase enzyme leading to accumulation of acetylcholine at neuromuscular junctions and synapses
Organophosphate Poisoning • Very potent agricultural insecticides and lethal war weapons. • Very easily absorbed through all parts of the skin. • Inhibit the enzyme and cause accumulation of ACh at all sites.
Treatment of Organophosphate Poisoning • Stop the exposure, wash extensively, very lipid soluble. • Atropine, a parasympatholytic drug, in very large doses, until the appearance of Atropine Poisoning. • Pralidoxime, when given very early after the poisoning, can regenerate the enzyme.