Download
1 / 31
350 likes | 574 Vues
Endocrine Hypertension and Adrenal Incidentalomas. Goals and Objectives. Review indications for secondary workup of hypertension Discuss major Endocrine causes for hypertension Screening and confirmatory testing Localization Treatment Discuss evaluation of adrenal incidentalomas

E N D
Goals and Objectives • Review indications for secondary workup of hypertension • Discuss major Endocrine causes for hypertension • Screening and confirmatory testing • Localization • Treatment • Discuss evaluation of adrenal incidentalomas • Initial diagnostic workup • Indications for surgery or biopsy • Long-term monitoring schedules
Secondary Hypertension • 2006 AACE Guidelines • Suspect secondary cause: • Sudden onset, intermittant, especially labile • Contributing factors absent • Abnormal clinical or lab features • Cushingoid habitus • Hypokalemia • Resistant to therapy • Uncontrolled with 3 medications including diuretic
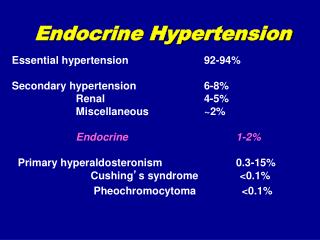
Primary Hyperaldosteronism • Incidence varies • Overall 6.1% • Stage 1 (<160/<100) 2% • Stage 2 (<180/<110) 8% • Stage 3 (>180/>110) 13% • Diagnostic clues • Hypokalemia (spontaneous or diuretic-induced) • Hypomagnesemia • Metabolic alkalosis
Primary Hyperaldosteronism • Indications for screening • Stage 2/3 HTN (BP >160/>100) • Resistant HTN (BP >140/>90 despite 3 BP meds) • 17-23% prevalence • Spontaneous or diuretic-induced hypokalemia • HTN with adrenal incidentaloma • 1-10% prevalence
Primary Hyperaldosteronism • Screening test • Aldosterone concentration (ng/dL):plasma renin activity (ng/mL/h) ratio • “Aldo renin ratio” or “ARR” • >20 • >30 • >40 • +/- Aldosterone concentration >15ng/dL • 16-37% of primary hyperaldo patients have aldo of 9-16ng/dL
Primary Hyperaldosteronism • Confirmatory tests • Saline load • Aldosterone remains >7ng/dL • Oral salt load • Ensure normal serum potassium • 2g sodium chloride TID for 4 days • 24-hr urine aldosterone on day 4-5 >12mcg/24-hr • Fludricortisone suppression test • Ensure renin activity <1ng/mL/h • Serum aldo >6ng/dL • Captopril challenge • <30% aldo suppression from initial level
Primary Hyperaldosteronism • Localization • Adrenal CT scan • Better spatial resolution than MRI • Adrenal venous sampling Young, W, et al. “Role for adrenal venous sampling in primary aldosteronism.” Surgery, 2004;136:1227-35.
Primary Hyperaldosteronism • Treatment • Goals • Normalize potassium • Normalize BP • Antagonize aldosterone’s effect on endothelium
Primary Hyperaldosteronism • Treatment • Adrenalectomy • Only for aldosterone producing adenomas (APA) or unilateral adrenal hyperplasia (UAH) • Medical therapy • Spironolactone • Eplerenone if limited by side effects • Amiloride, triamterene, ACE-I/ARB’s • (<1% of hyperaldo cases due to glucocorticoid-remediable aldosteronism) • (Usually suggested by FHx of HTN <20yo and hemorrhagic CVA) • (Diagnosed by genetic testing) • (Dexamethasone or prednisone in lowest effective doses)
Pheochromocytoma • Rare, mostly benign tumors of adrenal medulla • 2-8 cases per million per year • 10% extradrenal (“paragangliomas”) • 10% bilateral • 10% recur after initial treatment • 10% malignant • May be episodic or part of familial syndrome • HTN may be episodic or sustained • Symptoms include • Palpitations • Headaches • Diaphoresis • Orthostatic hypotension
Lenders, J, et al. “Biochemical diagnosis of pheochromocytoma: which test is best?” JAMA. 2002. 287(11):1427-34. Sensitivity: Specificity: • Multicenter cohort study of 214 patients with confirmed PC and 644 patients determined to not have PC • Plasma fractionated metanephrines (99%) • Urinary fractionated metanephrines (97%) • Urinary catecholamines (86%) • Plasma catecholamines (84%) • Urinary total metanephrines (77%) • Urinary VMA (64%) • Urinary VMA (95%) • Urinary total metanephrines (93%) • Plasma fractionated metanephrines (89%) • Urinary catecholamines (88%) • Plasma catecholamines (81%) • Urinary fractionated metanephrines (69%)
Lenders, J, et al. “Biochemical diagnosis of pheochromocytoma: which test is best?” JAMA. 2002. 287(11):1427-34. Sensitivity: Specificity: • Multicenter cohort study of 214 patients with confirmed PC and 644 patients determined to not have PC • Plasma fractionated metanephrines (99%) • Urinary fractionated metanephrines (97%) • Urinary catecholamines (86%) • Plasma catecholamines (84%) • Urinary total metanephrines (77%) • Urinary VMA (64%) • Urinary VMA (95%) • Urinary total metanephrines (93%) • Plasma fractionated metanephrines (89%) • Urinary catecholamines (88%) • Plasma catecholamines (81%) • Urinary fractionated metanephrines (69%)
Pheochromocytoma • Labs can be affected by: • Other medications • TCA • Antipsychotics • Levodopa • Amphetamines • Clonidine withdrawal • Phenoxybenzamine • Decongestants • Ethanol • Acetaminophen • Physical stressors • Stroke • Major operation • Myocardial infarction • Heart failure • Obstructive sleep apnea
Algorithmic Approach to Diagnosis • Determine if clinical suspicion is high • Past h/o treated PC and recurrent HTN or dizziness • FH of PC • MEN2 or other genetic syndrome • Von HippelLindau • Neurofibromatosis type 1 • Familial paraganglioma • Incidental adrenal mass with suggestive characteristics • High Hounsfield unit density • Delayed washout <50% in 10min • High intensity on T2 • Cystic and hemorrhagic changes • Bilateral • Large size >4cm)
Pheochromocytoma • Treatment • Volume expansion • Medications • Alpha Blockers • Phenoxybenzamine • Prazosin • Later BB’s or CCB’s (or both) • Surgical excision • Curative in 75% of cases • Can be done laparoscopically if • Tumor <6cm • No evidence of invasion into adjacent tissue • No regional or metastatic disease • Normal contralateral adrenal gland
Cushing’s Syndrome • Uncommon secondary cause of HTN • 75% have HTN • Subjective/objective findings • Centripetal obesity • Supraclavicular fat pad • Facial plethora • Hirsutism • Acne • Widened, purple striae • Glucose intolerance • Hypokalemia • Hypomagnesemia • Metabolic alkalosis
Cushing’s Syndrome • Diagnosis • Low dose DXM suppression (serum cortisol >5μg/dL) • 24-hr urine cortisol >50μg • Late night salivary cortisol >145ng/dL • Midnight serum cortisol >1.8μg/dL • Localization • ACTH or non-ACTH mediated • ACTH >5pg/mL • High dose (8mg) DXM suppression • Inferior petrosal vein sampling
Cushing’s Syndrome • Treatment • Surgical • Adrenalectomy • Trans-sphenoidal pituitary adenoma excision • (Bilateral adrenalectomy) • Medication • Ketoconazole • Mitotane
Other Hormonal and Enzymatic Causes for HTN • Adrenal • Enzyme deficiencies • 11β-hydroxylase • 17α-hydroxylase • 11β-hydroxysteroiddehydrogenase • 11-Deoxycorticosterone secreting tumors • Thyroid • Hyper- and hypo-thyroidism • Hyperparathyroidism • Pituitary • Acromegally • Renal • Renin-secreting tumor • Fibromuscular dysplasia • Renal artery stenosis • Liddle syndrome • Hypokalemia • Metabolic alkalosis • LOW aldosterone • Pregnancy • Gestational HTN • Eclampsia/HELLP • Hydatidiform mole
Adrenal Incidentalomas • Glomerulosa • Aldosterone • Fasciculata • Cortisol • Reticularis • DHEA • Androstenedione • Medulla • Epinephrine • Norepinephrine • Dopamine
Adrenal Incidentalomas • Definition • Unsuspected mass found on imaging • Incidence in autopsy series 8.7% • Diagnostic considerations • 1. Is the mass hormonally active? • 80% nonfunctioning • 5% subclinical Cushing Syndrome • 5% Pheochromocytoma • 1% aldosterone-producing adenoma (Conn’s tumor) • 2. Does it have worrisome radiologic features for malignancy? • 5% adrenocortical carcinoma • 3. Does the patient have a previous history of a malignant lesion? • 2.5% metastatic malignancies • Most commonly Lung, breast, stomach, kidney, melanomas, lymphomas
History and Physical • History • Weight change • Easy bruising • New HTN • New DM • Proximal muscle weakness • Edema • Fatigue • Virilization • Headaches • Anxiety • Sweating • Palpitations • Pallor • Low potassium • “B” symptoms • History of cancer • Current/prior smoking • Family history of Endocrine tumors or other cancers • Physical • Blood pressure • Pulse • Central obesity • Dorsocervical/supraclavicular fat pad • Facial plethora • Hirsutism • Acne • Ecchymoses • Striae • Muscle wasting
Suggested Evaluation • Biochemical evaluation • Cushing’s Syndrome • 1mg DXM suppression test • 24-hr urine free cortisol • Pheochromocytoma • Plasma fractionated metanephrines • 24-hr urine total metanephrines and fractionated catecholamines • Aldosterone concentration:plasma renin activity ratio • Only if hypertensive
Suggested Evaluation • Imaging • High resolution adrenal CT with contrast • Benign features • <10HU on noncontrast CT • 80-90HU with >50% washout on contrast CT • Pheochromocytomas generally enhance to >100HU • T2-weighted adrenal MRI • Benign features • High-signal enhancement on T2 • Highly characteristic of pheochromocytoma
Surgical Indications • Any lesion with concerning radiographic features • Most lesions >4cm • <4cm = 2% risk of malignancy • 4.1-6cm = 6% risk • >6cm = 25% risk • Unilateral hormone-producing adenomas • Except “Subclinical” Cushing’s Syndrome • Normal physical appearance, BP, potassium, insulin sensitivity, BMD • New hormonal activity or >1cm growth
Perioperative Management • Adrenocortical carcinoma • Full hormonal assessment • Open adrenalectomy recommended • Cortisol-producing adenoma • Rule out pheochromocytoma • Glucose and BP management • DVT and UGIB prophylaxis • Postoperative hydrocortisone • Pheochromoctyoma • Alpha blockade 1-3 weeks preoperatively • Long-term biochemical monitoring for recurrence • Aldosterone-producing adenoma • Rule out pheochromocytoma • BP, potassium, magnesium management
Long-term Monitoring of Adenomas • Biochemical • Annual for 5yrs • Risk of becoming hormonally active at 1, 2, and 5yrs • 17%, 29%, and 47%, respectively • Cushing’s Syndrome most likely to develop • Imaging • Re-assess size at 3-6mo • Annual for 1-2yrs • Risk of enlarging at 1, 2, and 5yrs • 6%, 14%, and 29%, respectively
References • Funder, J, et al. “Case detection, diagnosis, and treatment of patients with primary hyperaldosteronism: an Endocrine Society clinical practice guideline.” J ClinEndocrinol and Metab, 2008;93(9):3266-81. • Nieman, L, et al. “The diagnosis of Cushing’s Syndrome: an Endocrine Society clinical practice guideline.” J ClinEndocrinol and Metab, 2008;93(5):1526-40. • Torre, J, et al. “American Association of Clinical Endocrinologists medical guidelines for clinical practice for the diagnosis and treatment of hypertension.” Endo Pract, 2006;12(2):193-222. • Young, W, et al. “Role for adrenal venous sampling in primary aldosteronism.” Surgery, 2004;136:1227-35. • Zeiger, M, et al. “American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons medical guidelines for the management of adrenal incidentalomas.” Endo Pract, 2009;15(Suppl 1):1-20.