Download
1 / 24
250 likes | 792 Vues
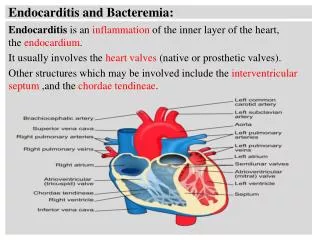
Endocarditis and Bacteremia:. Endocarditis is an inflammation of the inner layer of the heart, the endocardium . It usually involves the heart valves (native or prosthetic valves).

E N D
Endocarditis and Bacteremia: Endocarditis is an inflammation of the inner layer of the heart, the endocardium. It usually involves the heart valves (native or prosthetic valves). Other structures which may be involved include the interventricular septum ,and the chordae tendineae.
a Endocarditis is characterized by a prototypic lesion, the vegetation, which is a mass of platelets, fibrin, microcolonies of microorganisms, and inflammatory cells. . Picture of a granuloma (without necrosis) as seen through a microscope on a glass slide. The granuloma in this picture was found in alymph node of a patient With Mycobacterium avium infection .
a The simplest classification of endocarditis is based on : Etiology:infective or non-infective, depending on whether a microorganism is the source of the inflammation or not.
Infective endocarditis: Since the valves of the heart do not receive any dedicated blood supply, defensive immune mechanisms cannot directly reach the valves via the bloodstream. If an organism (such as bacteria) attaches to a valve surface and forms a vegetation, the host immune response is blunted. Normally, blood flows smoothly through these valves. If they have been damaged (from rheumatic fever, for example) the risk of bacteria attachment is increased.
A The endothelial lining of the chambers of the heart and blood vessels is resistant to bacterial infection. Endothelial damage however, for example from a "jet lesion" caused byinvoluntary return of blood flow, may produce a localized, sterile vegetation of platelets and fibrin. This may then allow circulating micro-organisms to adhere to the valve. Once attached, the bacteria may become enclosed in fibrin and platelets and multiply rapidly.
a Infected vegetations (lesion)occur along the edges of the heart valves, on the ventricular side for mitral and aortic valve and on the atrial side in tricuspidvalve. Left sided endocarditis are most common, accounting for 95% of cases. Rightsided endocarditis accounts for 5% of cases and is most often seen due to IV drug fluid invasion or in the immunosupressed patients; the tricuspid valve is affected and the organism is usually a Staphylococcus.
N Prosthetic valve endocarditis results from infection of a prosthetic valve. This may occur early, within 60 days of surgery, either during the operation or due to a perioperative bacteremia (urinary catheterization).
Types of infective endocarditis: Infective endocarditis has been classified into two broad categories according to the pathogenic organism and the clinical presentation: 1-Acute: Most often caused by Staphylococcus aureus. Equally prevalent on normal and abnormal valves. It is rare. 2-Subacute: Most often caused by Streptococcus viridans . Usually affects normal, and abnormal valves. More common.
Incidence of endocarditis: Acute form: Incidence of infective endocarditis in Europe and the USA is around 1.7-6.2 per 100,000 person-years. Twice as common in men than in women. Average mortality rate is 20%: Higher in patients over 65 years of age 0.1% of all cardiac deaths. Subacute infection far more prevalent than acute form. 50% of cases occur on normal valves, 15-30% of cases occur on prosthetic heart valves. Left sided endocarditis accounts for 95% of cases, aortic and mitral valves are effected equally.
In the subacute form of infective endocarditis, the vegetation also include a center of granulomatous tissue, which may undergo fibrosis (collagen) or calcification
Non-infective endocarditis: This form occurs more often in patients with Lupus erythematosus and is thought to be due to the deposition of immune complexes. These immune complexes precipitate an inflammation reaction, and it involves small sterilevegetations.
Diagnosis of endocarditis is based on the clinical features, investigations such as echocardiogram, as well as any blood cultures demonstrating the presence of endocarditis-causing microorganisms.
Bacteremia: Bacteremia is the presence of bacteria in the blood. The blood is normally a sterile environment, so the detection of bacteria in the blood (most commonly with blood cultures) is always abnormal. Bacteria can enter the bloodstream as a severe complication of infections (like pneumonia), during surgery (especially when involving mucous membranes such as the gastrointestinal tract), or due to catheters and other foreign bodies entering the arteries or veins (including intravenous drug).
N The immune response to the bacteria can cause sepsis and septic shock. Septic shock is a medical emergency caused by decreased tissue perfusion and oxygen delivery as a result of severe infection and sepsis. It can cause multiple organ dysfunction syndrome and death. Themortality rate from septic shock is approximately 25%-50%. The Gram negative lipopolysaccharide (Endotoxin) bind to LPS-binding protein which crosslink CD14 in blood.
a Blood monocyte, and neutrophils have CD14 receptors that discriminate the complexes. It will initiate cytokines production such as: TNF alpha, and IL-1 that will induce the following: 1- Decreased synthesis of anticoagulation factors such as tissue factor pathway inhibitor and thrombomodulin. 2- Systemic vasodilatation , edema, chemotaxis, endothelial injury and activation of leukocyte adhesion to the endothelial tissue.
a Bacteremia is different from sepsis (so-called blood poisoning or toxemia), which is a condition where bacteremia is associated with an inflammatory response from the body ( characterized by rapid breathing, low blood pressure, fever, etc.). Causes: In the hospital, indwelling catheters are a frequent cause of bacteremia and subsequent nosocomial infections, because they provide a means by which bacteria normally found on the skin can enter the bloodstream.
a Other causes of bacteremia include dental procedures , herpes , urinary tract infections, peritonitis, Clostridium difficilecolitis, and intravenous drug use. Sources of Bacteremia: 1-Gastrointestinal infection: Typhoid fever (Salmonellosis), Malta fever (Brucellosis), Yersinia infection and Bacteroidfragilis.
n 2-Genitourinary tract infection: Staphylococcus aureus, E.coli, Klebsiella, Citrobacter, Enterobacter, and Pseudomonus species. Treponema pallidum, Neisseria gonorrheae, 3-Respiratory tract infection: Neisseria meningitidis, H. influenza, Streptococcus pneumoniae, MRSA, VRE, and Klebsella pneumonia.
Diagnosis of acute and sub-acute endocarditis: Blood culture: A-5-8 ml blood should be extracted for culture. B-Specimens should be extracted during fever stage. C-Inoculation of blood culture bottle, and incubation under aerobic and anaerobic conditions. D- At 37˚C, blood should be incubated up to 8 days.
Blood culture results: Growth indicators: 1-Turbidity of blood culture media. 2-Air bubbles formation in the media. 3-Hemolysis of cultivated blood .
Identification of pyogenic Cocci from Blood culture (endocarditis): n
Staphylococcus aureus and Streptococcus viridans: Staphylococcusaureus species is DNase and Coagulase positive.
n Streptococcusviridansspeceis are resistant to Optichin and insoluble in bile salt.