Calcifications: think neuroendocrine
190 likes | 379 Vues
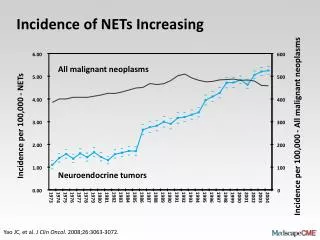
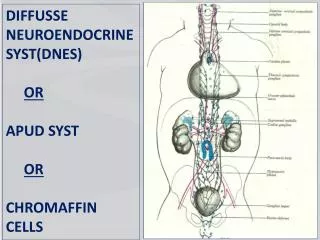
stent. SMV. SMV. SMA. Calcifications: think neuroendocrine. Biology of Tumor Detailed Knowledge of Pertinent Anatomy Goals of the Operation. 1.0. 1.0. 0.8. 0.8. 0.6. 0.6. Survival. 0.4. 0.4. 0.2. 0.2. 0.0. 0.0. 0. 2. 4. 6. 8. 10. 12. Years From Diagnosis.

Calcifications: think neuroendocrine
E N D
Presentation Transcript
stent SMV SMV SMA Calcifications: think neuroendocrine • Biology of Tumor • Detailed Knowledge of Pertinent Anatomy • Goals of the Operation
1.0 1.0 0.8 0.8 0.6 0.6 Survival 0.4 0.4 0.2 0.2 0.0 0.0 0 2 4 6 8 10 12 Years From Diagnosis Non Functional Islet Cell Tumors of Pancreas Overall survival n=162 patients Median survival: 3.2 yrs Five year survival: 43%
Survival: localized vs. metastatic disease — Median: 7.1 yrs ---Median: 2.1yrs p<0.0001 Localized(n=62) Metastatic (n=100)
NE Tumors of Pancreas • Biology of Tumor • Localized disease completely resected - - long medial survival (7.1 years) • Locally advanced disease - - surprisingly long median survival (5.2 years) • Metastatic disease - - short median survival (< 2 years) • Detailed Knowledge of Pertinent Anatomy • Goals of the Operation
PV Splenic V SMV Ileum Jejunum Proximal SMV Anatomy
Anatomy during Surgical Removal Vein resection Islet cell tumor in pancreatic head SMV SMA Vein graft
PV Splenic V SMV Ileum Jejunum First jejunal branch from the SMV – relationship to the uncinate prrocess
NE Tumors of Pancreas • Biology of Tumor • Localized disease completely resected - - long medial survival (7.1 years) • Locally advanced disease - - surprisingly long median survival (5.2 years) • Metastatic disease - - short median survival (< 2 years) • Detailed Knowledge of Pertinent Anatomy • SMV and its major branches • Relationship of pancreas to SMV and SMA • Goals of the Operation
What about Locally Advanced Tumors? T T SMV PATH: NEUROENDOCRINE CARCINOMA, LOW GRADE.
FAS in the Treatment of Patients With Locally Advanced PNET • 40% of patients with advanced or metastatic PECs respond to the FAS • median interval to response ~ 4 months • patients with SD at 6 to 8 weeks should continue for at least four cycles. • chromogranin A useful surrogate marker for the response to chemotherapy Kouvaraki,JCO, 2004: pp. 4762-4771
NED x 2.5 years DISTAL SUBTOTAL PANCREAS AND SPLEEN, RESECTION: WELL-DIFFERENTIATED (LOW-GRADE) PANCREATIC ENDOCRINE CARCINOMA OF TAIL OF PANCREAS, MEASURING 10.0 CM IN LARGEST DIMENSION, EXTENDING INTO THE PERIPANCREATIC SOFT TISSUE, SPLENIC VEIN, SPLENIC HILUM, AND INTO THE GASTRIC WALL. METASTATIC WELL-DIFFERENTIATED PANCREATIC ENDOCRINE CARCINOMA IN SIX OF TEN PERIPANCREATIC AND SPLENIC HILAR LYMPH NODES (6/10).
What about patients with metastatic disease ? Primary tumor (calcifications) Metastatic islet cell CA embolization - chemo - surgery E 474820
Removing the Primary Tumor When Metastases are Present — Median: 3 yrs --- Median: 1.8 yrs p=0.06 Resected (n=16) BUT! This may not apply to a patient with low volume DM and a primary in the pancreatic head Hard to justify resection of the primary tumor in the presence of unresectable distant metastases Not resected (n=80)
Nonfunctioning Islet Cell CA Localized potentially resectable NF islet cell CA (if low volume metastatic disease is likely-consider in operative plan) resect primary even if DM if DM: open-close anticipate complications from the primary will require extended resection age, co-morbidity favorable advanced age, cardiac disease laparotomy laparoscopy if positive consider chemo Primary in the pancreatic head with biliary obstruction and impending gastric outlet obstruction
NE Tumors of Pancreas • Biology of Tumor • Localized disease completely resected - - long medial survival (7.1 years) • Locally advanced disease - - surprisingly long median survival (5.2 years) • Metastatic disease - - short median survival (< 2 years) • Detailed Knowledge of Pertinent Anatomy • SMV and its major branches • Relationship of pancreas to SMV and SMA • Goals of the Operation • Combined resection of primary and metastatic tumor rarely possible • Palliative resection of pancreatic head in patients with low volume metastasis may be helpful-avoid observing these • Avoid surgery-related mortality and major morbidity in patients with locally advanced disease
Nonfunctioning Islet Cell Carcinoma • Anticipated changes in treatment algorithms • Improved systemic therapy • ? Expanding role of liver transplantation • Will require improved control of the primary tumor • (may alter current treatment recommendations)