Download
1 / 59

E N D
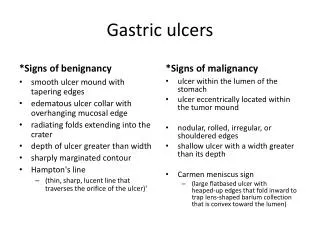
12 year old female presents to ER with confusion of 2 days duration with a fever. No family present to give history. No known past medical problems. On exam, she is 150 pounds, a temp of 39.5, and blood pressure of 90/60. She is obtunded. There are no skin rashes or meningeal signs. Fundi are normal. Cardiopulmonary exam is unremarkable. Lab studies show a HCT of 21, platelet count of 20K, BUN of 80, and creatinine of 3.0. Reticulocyte count is mildly elevated at 4.0%, with an elevated LDH of 700U/L. Chest X-ray is unremarkable. EKG is sinus tachycardia.
PT and pTT are normal. D-dimer is negative with normal fibrinogen level. Head CT was negative for intracranial bleed. Lumbar puncture was not performed secondary to low platelet count. Broad spectrum antibiotics were started to cover for meningitis and possible sepsis. Patient is given a 2L NS bolus and quickly rushed to the PICU. The fellow advises you to go look at the smear while he/she stabilizes patient. Smear is as shown.
Thrombotic MicroangiopathiesA clearer picture ahead?Daniel C WilliamsSenior PresentationJanuary 31, 200
Thrombotic microangiopathies are microvascular occlusive disorders that are a common pathway of different pathological processes. Such disorders are characterized by systemic or intrarenal aggregation of platelets and/or fibrin, mechanical injury to red blood cells, and thrombocytopenia.
Thrombotic Thrombocytopenia Purpura“Classic Signs” • Fever • Thrombocytopenia • Neurological abnormalities • Microangiopathic hemolytic anemia • Renal dysfunction
Hemolytic Uremic Syndrome“Classic Signs” • Thrombocytopenia • Renal dysfunction • Microangiopathic hemolytic anemia -Pancreatitis and seizures are common extra-renal complications which occur in approximately 20-30% of patients
Thrombotic Thrombocytopenia Purpura • Four general types exist: -infantile -acquired -drug induced -systemic disease • Overall incidence is low with approximately 3.7 cases/1,000,000 population.
Familial TTP • May appear in infancy or early childhood • Recurs at monthly intervals • Prognosis very poor • Caused by a deficiency of ADAMST13, an endothelial protease
Acquired TTP • Usually occurs in adults and children, with a peak in the second decade of life • Is sporadic and characterized as a single acute episode, although recurrences can occur • Thought to be caused by an autoantibody to ADAMST13
Drug-Induced TTP • Quinine typically most common • Anti-platelet agents ticlopidine and clopidogrel have been associated with TTP presenting in adults • Mechanism of action unknown, except quinine know to induce autoantibody against platelets
Systemic Disease Associated with TTP • Adenocarcinoma of Stomach / Pancreas / Prostate • Antiphospholipid Antibody Syndrome • Systemic Lupus Erythematosus • Pregnancy/Contraception • AIDS
Hemolytic Uremic Syndrome • Diverse group of disorders -Inherited -Post-Infectious -Drug related -Thrombotic Microangiopathy
Post-Infectious HUS • Most common cause of renal failure in children less than 4 years of age, epidemic cases are associated with a bacterial protein referred to as a shiga toxin • Organisms most commonly associated- E. Coli 0157:H7, shigella dysenteria type 1, and rare cases of Streptococcus pneumonia (mechanism not currently known) • 9 to 30% of patients with E. Coli 0157:H7 infection progress to having HUS
Hemolytic Uremic Syndrome • In the state of North Carolina, the average number of reported E. Coli 0157:H7 cases per year from 1997-2000 was 97. • Beef and cattle are the main reservoir, with risk of transmission greatest when ingesting uncooked or partially cooked meat and/or unpasteurized dairy products.
Post-Infectious HUS- Strep. Pneumonia • Usually have a poorer clinical outcome in comparison to shiga toxin induced HUS • A study in Pediatrics 2000 found that children were younger (22.1 vs. 49 months), more likely to require dialysis (75 vs. 49%), had longer hospital stays (33.2 vs. 16.1 days), and received more platelet and red blood cell transfusions.
Post-Infectious HUS- Strep Pneumonia • Mechanism of underlying HUS unknown. • Plasma exchange should be avoided secondary to plasma containing antibodies against the Thomsen-Friedenreich antigen, which could accelerate polyagglutination and hemolysis.
Inherited HUS- Factor H deficiency • Relatively common cause of HUS and accounts for approx. 5-10% of all cases • Factor H is an important enzyme in the complement cascade, which when absent, allows unregulated complement mediated cell lysis • Such cell lysis is preferentially localized to glomerular endothelial cells causing the symptom complex of HUS
Drug Induced HUS/TTP • Associated with immunosuppressants cyclosporine, tacrolimus and is a seen side effect after allogenic bone marrow, kidney, liver, heart, and lung transplantation. • OKT3 implicated in transplanted kidneys found to have evidence of HUS • Occurs after prolonged combination chemotherapy and total body irradiation, with mitomycin and cisplatin common agents implicated • Mechanism of these microangiopathies unknown
Pathophysiology of TTP • More well defined • Microvascular thrombi consist only of platelet aggregates. • No perivascular or endothelial cell damage. • Platelet aggregates contain abundant von Willebrand factor multimers, which are the precleaved form of vWf antigen and bind platelets at the glycoprotein 2B/3A receptor with high affinity.
Pathophysiology of TTP: • A metalloprotease enzyme (ADAMS T13) is usually produced by hepatocytes, binds to endothelial cells by a thrombospondin receptor, and cleaves vWf multimers to produce monomers with a low affinity for platelet binding.
Proposed Mechanism of HUS • Infection by a microbe which releases a 70-kD protein referred to as a “shiga toxin” is a presumed requirement. • Shiga toxin is of a singular A subunit, and 5 B subunits • The B subunit of shiga toxin binds to globotriaosylceramide (Gb3) receptors, present in glomerular, colonic, cerebral, endothelial, renal mesangial and tubular cells, and platelets.
Proposed Mechanism of HUS • Shiga toxin binds by the B subunit to colonic epithelia, generating an intense inflammatory response mediated by neutrophils and interleukin-8. • Higher initial WBC is thought to be a predictor of worse outcome because of the intense neutrophil response. • Binding of the shiga toxin allows bacterial entrance to mucosal cells causing cell death and exposing underlying vasculature.
Proposed Mechanism of HUS • Shiga toxin crosses into the circulation and travels by platelets/monocytes to bind to glomerular, mesangials, and renal tubular epithelial cells. • Toxin stimulated renal epithelial cells may secrete unusually large multimers of vWf that then bind toxin activated platelets. • ADAMTS 13 activity is thought to be impaired secondary to interaction with Gb3 receptors on endothelial cells.
Proposed Mechanism of HUS • Endocytosis of subunit A of the shiga toxin may cause death and desquamation of endothelial cells. • Epithelial cell death exposes underlying large vWf multimers along with tissue factor which precipitates clotting cascade. • Activation of the clotting cascade and production of fibrin is thought to be key difference between TTP and HUS.
HUS- Why the Kidneys? • Gb3, the glycolipid receptor responsible for binding the B subunit of shiga toxin, is expressed 50X more in kidney than in the endothelial cells of lung or liver. • The shiga toxin appears to stimulate release of TNF from kidney cells in vitro, which may in turn stimulate increased production of Gb3 further potentiating injury.
Prothrombotic Abnormalities of HUS • Evidence exists that a prothrombotic state is generated prior to development of the renal dysfunction associated with HUS. • 53 children infected with E. Coli 0157:H7 were studied for evidence of prothrombin fragment 1+2, tissue plasminogen activator antigen (t-PA), tPA-plasminogen activator inhibitor type 1(PAI-1) complex, and d-dimer.
Prothrombotic Abnormalities of HUS • 16 of the 53 children went on to develop HUS, ranging from day 5-13 of illness • Blood was drawn on day 4 of diarrheal illness, regardless of whether HUS develops • Urine samples were tested for evidence of Beta-2 microglobulin as well as N-acetyl-Beta-glucosaminidase, both early markers of renal tubular cell damage.
Baboon Model for HUS • Baboons received either 1 dose of 100ng/kg Shiga Toxin-1 or 4 doses of 25ng/kg Shiga Toxin-1 separated by 6 hours. • The 6 animals that received the single dose of shiga toxin all developed thrombocytopenia, acute renal failure, MAHA, and glomerular pathology of HUS. • Animals that received 4 divided doses of shiga toxin developed no signs of HUS, with no glomerular pathology noted.
Inherited HUS- Factor H Deficiency • A major contributor to familial HUS (5-10 percent of all cases) • Factor H, a 150 kD plasma protein, regulates the complement pathway by displacing Bb, from C3bBb, a catalytic enzyme of complement mediated cell lysis • Loss of protein Bb allows for degradation of C3b
Factor H Deficiency • Loss of Factor H function allows over expression of C3bBb, and potentiation of autoantibody and complement mediated damage to glomerular endothelium and sub endothelium.
Therapy of TTP/HUS: Plasma Exchange • Plasma exchange has become standard of care for all patients given the diagnosis of TTP. • Prior to plasma exchange, the 6 month mortality of patients with TTP was greater than 90%. • Goal is to rapidly reduce circulating levels of autoantibody against ADAMST13 and other possible prothrombotic compounds present in patients’ serum.
Therapy of TTP/HUS: Plasma Exchange • Venous blood is withdrawn and separated into blood cells and plasma. (plasmapheresis) • Separation occurs by centrifugation (intermittent or continuous), or by a membrane filter with a selective pore size for plasma. Blood cells cells are then mixed with FFP and given back to patient.
Therapy of TTP/HUS: Plasma Exchange • 210 adult patients with TTP were treated with either plasma exchange or plasma alone. • The 6 month survival was 78% for plasma exchange and 31% for plasma alone • Study was confounded secondary to those who underwent plasma exchange received 3X the amount of plasma.
Therapy of TTP/HUS- Plasma Exchange • High dose plasma exchange (25-30 cc/kg/day) was compared to first line plasma exchange at a single center. (2003) • 16/19 patients in HDPE group progressed to remission. (16/18 in PE group) • 6/19 patients in HDPE group were switched to PE group because of fluid overload and 2 because of unresponsiveness to therapy. (1/2 patients died) • 5/19 patients had nephrotic range proteinuria during treatment.
Therapy of TTP/HUS- Plasma Exchange • Complications • Bacteremia (10/71 patients) • Catheter Obstruction (7/71 patients) • Hemorrhage (2/71 patients) • Fungemia (2/71 patients) • Venous Thrombosis (2/71 patients) • Pneumothorax (2/71 patients)
Treatment of TTP/HUS • In comparison to TTP, HUS treatment is generally supportive with peritoneal dialysis if anuria lasts more than 48 hours or other indication for dialysis occurs • Spontaneous improvement of renal function with post-infectious HUS usually occurs in 1-2 weeks with mortality less than 5% • Peritoneal dialysis may be of additional help by removing procoagulant proteins from plasma.
Specific Therapies of HUS • A French prospective multicenter trial evaluated the benefits of FFP in 39 children, with 40 children who had supportive treatment used as control. • Plasma creatinine and urinary protein were higher at 6 months in the control group, but no difference noted at 12 months. • Late renal biopsy showed cortical necrosis in 7 of 10 control patients, but none in the plasma treated group.
Specific Therapy of HUS • Plasma exchange in the setting post-diarrheal HUS was studied in an E.Coli outbreak in Lankanshire, England. • 22 adults had HUS, 16 underwent plasma exchange and had a 69 percent survival rate. 6 had contraindications to plasma exchange and 0/6 survived.
Treatment of TTP/HUS- Alternatives? • 2 prospective trials evaluating the use of urokinase/heparin and dipyridamole/heparin were performed which no change in duration of renal failure, hemolysis, and thrombocytopenia. • IVIG was used in a controlled trial (400mg/kg for 5 days) with no difference in hemolysis, thrombocytopenia, and creatinine at one year.







![The signs of the times(2) [earthquakes]](https://cdn1.slideserve.com/2296340/the-signs-of-the-times-2-earthquakes-dt.jpg)