Download
1 / 47
480 likes | 919 Vues
Chapter 11. Supply Chain & Inventory Management. Outline. Healthcare Supply Chain Manufacturers/Suppliers Distributors, Wholesalers Group Purchasing Organizations (GPOs) e-Distributors Flow of Materials in Supply Chain Supply Chain Management Issues for Providers

E N D
Chapter 11.Supply Chain & Inventory Management Yasar A. Ozcan
Outline • Healthcare Supply Chain • Manufacturers/Suppliers • Distributors, Wholesalers • Group Purchasing Organizations (GPOs) • e-Distributors • Flow of Materials in Supply Chain • Supply Chain Management Issues for Providers • Contemporary Issues in Medical Inventory Management • Just-In-Time (JIT) & Stockless Inventories • Single vs. Multiple Vendors • Traditional Inventory Management • Requirements for Effective Inventory Management • Inventory Accounting Systems • Universal Product codes (UPCs) • Lead Time • Costs • EOQ Model • Reorder Point Yasar A. Ozcan
In healthcare organizations, supply chain is a new way of conceptualizing medical supply management. A supply chain is defined as “a virtual network that facilitates the movement of product from its production, distribution and consumption” (McFadden and Leahy, 2000). Healthcare Supply Chain Yasar A. Ozcan
Need for Healthcare Supply Chain Management • Improve operations • Increasing levels of outsourcing • Increasing transportation costs • Competitive pressures • Increasing globalization • Increasing importance of e-commerce • Complexity of supply chains • Manage inventories Yasar A. Ozcan
Figure 11.1 Healthcare Supply Chain Pharmaceutical Medical-Surgical Devices Manufacturers/ Suppliers Upstream Wholesalers Group Purchasing Organization (GPOs) e-Distributors Distributors Hospitals Hospital Systems Physicians Integrated Delivery Networks (IDNs) Providers Downstream Patients/Individuals Employers Insurers HMOs Drug Benefit Agencies Government End Users Yasar A. Ozcan
Manufacturers/Suppliers. Manufacturers of medical supplies can be classified in three categories: • drugs/pharmaceutical, • medical-surgical supplies, and • devices. • Some manufacturers produce supplies in more than one • category or in all categories. Healthcare Supply Chain Yasar A. Ozcan
Well known pharmaceutical manufacturers include Abbott, Aventis Pharma, Bristol-Myers Squibb, Eli Lilly, Merck, GlaxoSmithKline, Hoffmann-La Roche, Janssen, Johnson & Johnson, Pfizer, Schering-Plough and Wyeth. Twenty-five percent of pharmaceutical products are distributed to providers (hospitals and other institutional settings) via distributors. Medical-surgical companies produce items such as injection syringes and needles, blood and specimen collection kits, hospital laboratory products, wound management products, and intravenous solutions. 3M, Abbot, Baxter, Johnson & Johnson are a few of the well known medical-surgical companies that sell majority of their products through distributors. Healthcare Supply Chain Yasar A. Ozcan
Medical devices can be described as very high priced, technologically sophisticated and advanced apparatus that are used for diagnosis and therapies. Medical devices include surgical and medical instruments And apparatus, orthopedic, prosthetic and surgical appliances (for example, shoulder, knee, and hip replacements), X-Ray apparatus, tubes, irradiation apparatus, electro-medical and electro-therapeutic devices. Dupuy, Ortho Biotech, Medtronic, and Zimmer are examples of the companies that manufacture such devices (Burns, 2002; p.244). Healthcare Supply Chain Yasar A. Ozcan
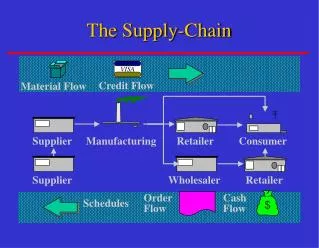
Supplier } Storage Service Patient Supplier Typical Supply Chain for a Healthcare Service Implants Replacement knee Replacement valve Operating Room Yasar A. Ozcan
Distributors for medical-surgical supplies are independent intermediaries who operate their own warehouses; they purchase the products from manufacturers/suppliers to sell to providers. Similarly, pharmaceutical intermediaries purchase the drugs/pharmaceuticals from manufacturers and wholesale them to pharmacies or to providers. Well known distributors of pharmaceuticals include AmriSource/Bergen Brunswig, Cardinal Health/Bindley Western and McKesson. The intermediaries are called distributor or wholesalers depending on whether the products’ final resale has another layer before reaching the customer (Burns, 2002; p.127). Cardinal Health, Owens&Minor, and McKesson are major distribution companies in hospital market. Distributors and Wholesalers Healthcare Supply Chain Yasar A. Ozcan
Electronic Data Interchange (EDI) Linking providers through electronic communication to their distributors is formally defined as electronic data interchange (EDI). EDI provides direct, real-time computer to computer electronic transmission of purchase orders, shipping notices, invoices and the like between providers and distributors. Over seventy-five percent of distributors use EDI, and seventy to eighty percent of their business volume is handled through EDI (Burns, 2002, pp.130-131). EDI is also proliferating to manufacturer transactions with other parts of the health care supply chain; more than one-third of their business transactions use EDI. The cost for standardized EDI transactions for a purchase order, as compared to costs with manual systems, saves operational costs for both providers and distributors. Healthcare Supply Chain Yasar A. Ozcan
0 214800 232087768 Electronic Data Interchange (EDI) • Increased productivity • Reduction of paperwork • Lead time and inventory reduction • Facilitation of just-in-time systems • Electronic transfer of funds • Improved control of operations • Reduction in clerical labor • Increased accuracy Yasar A. Ozcan
Group Purchasing Organizations (GPOs). Group purchasing organizations provide a critical financial advantage to providers, especially hospitals and hospital systems, by negotiating purchasing contracts for products and non-labor services. A typical GPO has many hospital organizations as its members and uses this as collective buying power in negotiating contracts with many suppliers: of pharmaceuticals, medical-surgical, supplies, laboratory, imaging, durable medical equipment, facility maintenance, information technology, insurance, food and dietary products and services. The contracts usually last three to five years, giving providers price protection (Burns, 2002, pp. 60-64). Healthcare Supply Chain Yasar A. Ozcan
Group Purchasing Organizations (GPOs). Over 600 GPOs operate in the United States; perhaps half of them focus their business on hospitals. The two largest GPOs are Novation and Premier, which are nonprofit.AmeriNet, HSCA and Consorta are the other sizable non-profit GPOs. The two investor-owned, for-profit GPOs are HCA/Health Trust and Tenet/BuyPower. A provider may be member of multiple GPOs. The average Hospital GPO membership ranges 1.6 to 2.6 GPOs in US. Healthcare Supply Chain Yasar A. Ozcan
e-Distributors. e-commerce in health care can be viewed from different perspectives. Here we will concentrate on two aspects: business to business (B2B) commerce and business to customer (B2C) commerce. Examples of B2B firms are: Medibuy, Neoforma, MedAssets, OmniCell, and Promedix. These firms provide e-Catalog, e-Request for Proposal (eRFP), e-Auction, and e-Specials. Healthcare Supply Chain Yasar A. Ozcan
Flow of Materials It is important to note that depending upon the type of medical supply, the flow of materials in the supply chain may take more direct routes to providers or end users. Suppliers may bypass GPOs by not contracting or negotiating price arrangements. High-end implants and medical devices, specialty items of low volume but high price, are good examples of such medical supplies for which suppliers use direct delivery, usually via express services (like FedEx, UPS, or DHL) or have their own local/regional sales representatives make the just-in-time (JIT) delivery and serve as consultants to physicians. In some cases, the company’s representatives provide technical participation with surgeons in implanting devices surgically. Other cases in which suppliers may bypass GPOs in contracting are for small-volume, esoteric items, and for the brand-name, specialty drugs used to treat cancer and cardiovascular problems. Healthcare Supply Chain Yasar A. Ozcan
Just-In-Time (JIT) and Stockless Inventories. Inventory management in healthcare organizations is becoming increasingly decentralized. JIT means that goods arrive just before they are needed. Stockless inventory means obtaining most of supplies from a single source (a prime vendor) in small packaging units ready to be taken to the user departments. Single versus Multiple Vendors.The essence of the purchasing function is to obtain the right equipment, supplies and services, and of the right quality, in the right quantity from the right source at the right price at the right time. Contemporary Issues in Medical Inventory Management Yasar A. Ozcan
Traditional Inventory Management Inventory Is. . . STOCK OR STORE OF GOODS Or Stock Keeping Items (SKUs) Yasar A. Ozcan
An Inventory Disaster! Imagine the following scenario, in which the healthcare supply chain manager has to explain to a member of senior management why the emergency room found itself without the syringes. ..Sorry sir, but when she (the patient) came into the ER,we were out of syringes. Our anticipation stockswere depleted because we hadn’t corrected the ordering patterns for seasonal variations. Then, the snow delayed shipments from supplier, and oursafety stocksjust weren’t good enough! You know we usually order in bulk to take advantages of large economic lot sizeand lower our ordering cycle. Our last order was especially large because we wanted to hedge against predicted price increases! In the final analysis, our inventory just wasn’t sufficient to permitsmooth operations… Yasar A. Ozcan
The COO’s Response(i.e., Inventory objectives and requirements) I hope you do realize that it is your duty to both maintain a high level of customer service and minimize the costs of ordering and carrying inventory! All I ask of you is that you make two fundamental decisions-- when to order and how much to order. Yasar A. Ozcan
Effective Inventory Management The requirementsfor effective inventoryinclude: • A system to keep track of inventory • A reliable forecast of demand • Knowledge of lead times and lead time variability • Reasonable estimates of inventory holding costs, ordering costs, and shortage costs • A classification system for inventory items Yasar A. Ozcan
Effective Inventory Management • Inventory counting systems can be either: • Periodic • Perpetual • Batch • Line Yasar A. Ozcan
Inventory Counting Systems • Periodic System Physical count of items made at periodic intervals • Perpetual Inventory System System that keeps track of removals from inventory continuously, thus monitoringcurrent levels of each item Yasar A. Ozcan
0 214800 232087768 Inventory Counting Systems (Cont’d) • Two-Bin System - Two containers of inventory; reorder when the first is empty • Universal Bar Code - Bar code printed on a label that hasinformation about the item to which it is attached Yasar A. Ozcan
0 214800 232087768 Inventory Counting Systems (Cont’d) Universal Product Codes (UPCs).The UPCs have been around since late 1970s and are used in industry. A UPC can have up to 20 character numbers that uniquely identify a product, for example, of pharmaceutical or medical-surgical supply, using bars with different variety and thickness that can be read by scanners. The order of the information in UPCs identifies the type of product, its manufacturer, and the product itself. Yasar A. Ozcan
Effective Inventory Management Universal Product Codes (UPCs). Only 26 percent of medical-surgical products can be scanned on nursing units, and only fifty percent of drugs have bar codes for unit doses. According to the final regulation issued by the Food and Drug Administration (FDA) in 2004, drug manufacturers must adopt bar coding to single-dose units within two years, and hospitals must eventually implement bedside scanning systems. The FDA estimates, however, that it may take up to two decades for all hospitals to implement such systems because of their high costs: from $.5 to $1 million. Only a few more than 100 hospitals currently them. Yet bar code systems would significantly improve the quality of patient care through reduction of medication errors. It is estimated that over a 20-year period, fully implemented bar code systems would prevent about .5 million medical errors. Moreover, by improving the cost-efficiency of medical supply management, hospitals would also reap $90 billion in savings, which would help to pay for the technology (Becker, 2004). Yasar A. Ozcan
Effective Inventory Management Lead Time Inventories are used to satisfy demand requirements, so reliable estimates of the amounts and timing of demand are essential. It is also essential to know how long it will take for orders to be delivered (Stevenson, 2002, p.547). Now that healthcare organizations increasingly rely on their vendors to maintain adequate inventory levels in their facilities, their data relevant to demand must be transferred to their vendors. Healthcare managers also need to know the extent to which demand and lead time (the time between submitting an order and receiving it) may vary; the greater the potential variability, the greater the need for additional stock to avoid a shortage between deliveries. Yasar A. Ozcan
Effective Inventory Management • Costs of Inventory: • Holding (carrying costs)-- interest, insurance, depreciation, obsolescence, deterioration, spoilage, pilferage, warehousing costs • Ordering costs-- associated with ordering and receiving inventory • Shortage costs-- when demand > supply on hand; opportunity costs of lost customers loss of goodwill; death of a patient and potential lawsuits Yasar A. Ozcan
60 40 20 % of Annual dollar volume 0 20 40 60 % of Items Effective Inventory Management The A-B-C Approach: Classifying inventory according to some measure of importance and allocating control efforts accordingly. A relative importance classification system • A - very important (15-20% of items; 60-70% of $$$s) • B - moderate • C - least important (60-70% of items; 10% $$$s) Tightest controls and management should be on A items A B C Yasar A. Ozcan
Table 11.1 A-B-C Classification Analysis Yasar A. Ozcan
EOQ Model ECONOMIC ORDER QUANTITY model-- It answers the question, “How much should I order?” by allowing you to determine an optimal order quantity in terms of minimizing the sum of certain annual costs that vary with order costs. Remember what the costs are? Yasar A. Ozcan
Figure 11.2 The Inventory Order Cycle for Basic EOQ Model Order Quantity, Q Cycle 1 Cycle 2 Cycle 3 Cycle 4 Q Depletion or Demand Rate Average inventory Level of Inventory (ROP) R 0 Time (days) Required safety stock Reorder Point Reorder Time Order Received Lead Time Yasar A. Ozcan
Q Average Inventory 0 Many orders, but low average inventory. Q 0 Average inventory level and number of orders per year are inversely related. WHY? 1 year Average Inventory Few orders but high average inventory. Yasar A. Ozcan
To refresh memory. . • Basic EOQ models minimize the sum of the holding and ordering costs of inventory. • Several assumptions are important to use for the model: • Only one product is involved • Annual usage (demand) requirements are known • Usage is spread evenly throughout the year so that usage rates are fairly constant • Lead time does not vary • Each order is received as a single delivery • There are no quantity discounts. Yasar A. Ozcan
Annual Cost Annual Cost Order Quantity Order Quantity Holding & Ordering Costs Conceptualized Q 2 D Q H S Ordering costs (S) are inversely and nonlinearly related to order size (Q). Carrying costs (H) are linearly related to order size (Q). Q 2 D Q Annual Carrying Cost = H Annual ordering costs = S Yasar A. Ozcan
Figure 11.3 The Economic Ordering Quantity Model Total cost Minimum TC Annual cost Holding cost QoFlexibility zone for Packaging requirements Ordering cost Order Quantity, Q Marginal cost for packaging requirements Economic Ordering Quantity (EOQ) Yasar A. Ozcan
EOQ Model ECONOMIC ORDER QUANTITY model-- It answers the question, “How much should I order?” by allowing you to determine an optimal Q0. Yasar A. Ozcan
Example 11.1: Syringe Inventory An orthopedic physician group practice uses 12cc syringes from Sherwood for their cortisone injections. During the each of last two years, 40000 of them were used in the office. Each syringe costs $1.50. The physician’s office annually discards, on average, 500 of the syringes that have became inoperable (broken, wrong injection material, lost). The syringes are stored in a room that occupies 2% of the storage area. The storage area constitutes 10% of the leased space. The annual office lease costs $60,000. The group practice can secure loans from a local bank at 6% interest to purchase the syringes. For each placed order, it takes about three hours for an office assistant (whose hourly wage is $9.00 and who receives $3.25 in fringe benefits) to prepare, and communicate the order, and place its shipment in storage. In addition, each order’s overhead share of equipment and supplies (phone, fax, computer, stationary paper) is approximately $4.50. In the past, the office assistant always placed 5,000 syringes in each order. The deliveries are made in boxes of 1000 syringes and are always received three working days after the order is placed. What should be the EOQ for the 12cc syringe? What are the inventory management costs for these syringes? What are the investment costs? How many times in a year should an order be placed? Yasar A. Ozcan
Solution: To calculate EOQ, we need to estimate the holding and ordering costs. Annual holding cost 1) Cost of inoperable syringes – 1.50 * 500 = $750. 2) Storage cost – (60000 Lease) * .10 (storage area) * .02 (syringe) = $120. 3) Interest on a loan used to purchase 5000 syringes: 5000 *1.5*.06 = $450. Total annual holding costs = 750 + 120 + 450 = 1320. Annual holding cost per syringe: 1320 ÷ 40000 = $.033. Ordering cost Office assistant’s time – 3 hours * (9.00+3.25) = $36.75. Overhead – $4.50. Total ordering cost – $36.75 + $4.50 = $41.25. Using formula the EOQ formula: Yasar A. Ozcan
Solution: Total inventory management cost calculated using formula: Investment cost: Investment costs = Order quantity * price of the item, or = Qo * p = 10000 * 1.50 = $15,000.00. Investment cost is the amount committed to purchase the syringes. It is cycled as the cost of the syringes is recovered from patients and/or third party payers. Order Frequency is calculated using formula: In other words, order frequency is four times a year. Yasar A. Ozcan
Summary The two decisions were how much to order, and when to order. To determine how much to order, you use an EOQ model that minimizes the sum of the total ordering and carrying costs. When to order? Should we order when you are almost out of inventory?! Yasar A. Ozcan
When to Order? • The reorder pointoccurs when the quantity on hand drops to a predetermined amount. • There are 4 determinants of the reorder point quantity: • Rate of demand • Length of lead time • Extent of demand and lead time variability • Degree of stock-out risk acceptable to management. • Demand Rates and Lead Times can be constant or variable. Yasar A. Ozcan
Constant Demand Rate and Lead Time There is no risk of a stock-out created by increased demand of lead times longer than expected. Thus, ROP equals the product of usage rate and lead time; no cushion stock is necessary. Example 11.2 An orthopedist surgeon replaces two hips per day. The implants are delivered two days after an order is placed, via express delivery. When should the supply chain manager order the implants? Solution: Usage = 2 implants daily. Lead Time = 2 days. ROP = Usage Lead Time = 2 * 2 = 4. Thus, order should be placed when 4 implants are left! Yasar A. Ozcan
Variable Demand Rates and/or Variable Lead Times Safety Stock-- stock held in excess of expected demand when demand rate and/or lead time is variable ROP = Expected demand during lead time + safety stock Example 11.3 A dentist office uses an average of 2 boxes of gloves (100-glove boxes) per day, and lead times average 5 days. Because both the usage rate and lead times are variable, the office carries a safety stock of 4 boxes of gloves. Determine the ROP. Solution: ROP = 2 boxes/daily 5 day lead time + 4 boxes ROP = 14 boxes. Yasar A. Ozcan
Variable Demand Rates and/or Variable Lead Times • Service Level--probability that demand will not exceed supply during lead time. • Service level is the complement of stock-out risk; 95% service level means a 5% risk of stock-out. • The greater the variability in either demand rate or lead time, the greater the amount of safety stock needed to achieve that service level. Yasar A. Ozcan
Summary Again • The two decisions were how much to order, and when to order. • To determine how much to order, you use an EOQ model that minimizes the sum of the total ordering and carrying costs. • When to order is determined by a reorder point model, and varies according to knowledge of lead times and demand. Yasar A. Ozcan
The End Yasar A. Ozcan