Download
1 / 64
730 likes | 2.1k Vues
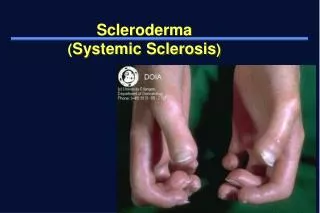
Scleroderma and Inflammatory Myositis. Kathryn Dao, MD Arthritis Center February 16, 2006. Scleroderma. “Skleros-” = hard “-derma” = skin Incidence 1-2/100,000 in USA Peak age of onset 30-50 y.o. Female:male 7-12: 1

E N D
Scleroderma and Inflammatory Myositis Kathryn Dao, MD Arthritis Center February 16, 2006
Scleroderma • “Skleros-” = hard “-derma” = skin • Incidence 1-2/100,000 in USA • Peak age of onset 30-50 y.o. • Female:male 7-12: 1 • Disease manifestation is a result of host factors + environment (concordance is similar in monozygotic and dizygotic twins)
Scleroderma Three major disease subsets: based on extent of skin dz • Localized Scleroderma • Morphea: manifests as focal patches • Linear scleroderma: band-like (linear) areas of thickening. (Coup de Sabre) • Limited disease AKA "CREST" syndrome • Calcinosis, Raynauds, Esophageal dysmotility Sclerodactyly, Telangiectasias • Diffuse disease - skin abnormalities extending to the proximal extremities (AKA - PSS) • (Scleroderma sine scleroderma)
DDX of Tight Skin • Pseudosclerodactyly • IDDM, Hypothyroidism • Drugs: Tryptophan, bleomycin, pentazocine, vinyl chloride, solvents • Eosinophilic fasciitis • Overlap syndromes • Scleredema
DDX of Tight Skin • Scleromyxedema (popular mucinosis) • Scleroderma-like conditions • Eosinophil myalgia syndrome (tryptophan) • Porphyria cutanea tarda • Toxic oil syndrome • Nephrogenic fibrosing dermopathy
ACR Systemic Sclerosis Preliminary Classification Criteria* • Major Criterion • Proximal Scleroderma • Minor Criteria • Sclerodactyly • Digital pitting or scars or loss of finger pad • Bibasilar pulmonary fibrosis * One major and two minor required for diagnosis
Scleroderma: Onset • Raynauds • Swollen or puffy digits • Loss of skin folds, no hair growth • Digital pulp sores/scars • Arthralgias >> Arthritis
SclerodermaA disorder of Collagen, Vessels • Etiology: unknown? • Autoimmune disorder suggested by the presence of characteristic autoantibodies such as ANA, anti-centromere and anti-SCL-70 antibodies. • Pathology: • Early dermal changes lymphocytic infiltrates primarily of T cells • Major abnormality is collagen accumulation with fibrosis.
SclerodermaA disorder of Collagen, Vessels • Small to medium-sized blood vessels, which show bland fibrotic change Vasculopathy, NOT vasculitis! • Small thrombi may form on the altered intimal surfaces. • Microvascular disease Cold Normal Cold PSS
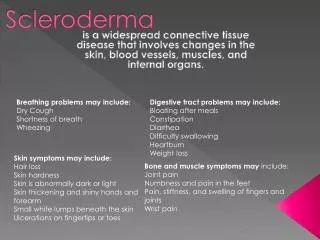
PSS - Clinical • Skin: • Skin thickening is most noticeable in the hands, looking swollen, puffy, waxy. • Thickening extends to proximal extremity, truncal and facial skin thickening is seen. • Raynaud's phenomenon is present. • Digital pits or scarring of the distal digital pulp • Musculoskeletal: Arthralgias and joint stiffness are common. • Palpable tendon friction rubs associated with an increased incidence of organ involvement. • Muscle weakness or frank myositis can be seen.
Skin Scores Extent of skin involvment predictive of survival: % Survival at 5 yr 10 yr Sclerodactyly 79-84 47-75 Truncal 48-50 22-26 J Rheumatol 1988;15:276-83.
PSS - Clinical • Gastrointestinal: Esophageal dysmotility, dysphagia, malabsorptive or blind loop syndrome, constipation.
Renal: Kidney involvement is an ominous finding and important cause of death in diffuse scleroderma. A hypertensive crisis (AKA renal crisis) may herald the onset of rapidly progressive renal failure.
Scleroderma Renal Crisis • Risk Factors • diffuse skin involvement • rapid progression of skin thickening • disease course < 4 years • anti-RNA-polymerase III-antibodies • newly manifested anemia • newly manifested cardiac involvement • pericardial effusion • heart insufficiency • preceded high-dose corticoid therapy • pregnancy Am J Med 1984;76:779-786.
Scleroderma Renal Crisis • Microangiopathic hemolytic anemia +Microscopic hematuria • Fatal before the introduction of ACE-I, CCB • Survival without ACE-I 16% @ 1 year, with ACE-I 45% at 5 years • Continue use of ACE-I even if dialysis appears imminent Ann Int Med 1990;113:352-357.
Pulmonary Manifestations of PSS • Dyspnea • Pulmonary HTN primarily in CREST • Ground glass (alveolitis) • Interstitial fibrosis (bibasilar) • High resolution CT vs Gallium Scan • Major cause of death • RARE: • Pulmonary embolism • Pulmonary vasculitis
PFT’s in Systemic Sclerosis • Decreased DLCO is the Earliest Marker • Increased A-a Gradient with Exercise • Restrictive Pattern • VC, FEV1/FVC • Pulmonary Vascular Disease • DLCO with Normal Volumes
Cardiac Findings in PSS • Myocardial fibrosis • Dilated cardiomyopathy • Cor pulmonale • Arrhythmias • Pericarditis • Myocarditis • Congestive heart failure • Myocardial infarction (Raynaud’s)
Feature LimitedCREST Diffuse PSS Calcinosis ++ + Arthralgia/Arthritis ++ ++++ Pulmonary fibrosis ++ +++ Pulmonary HTN ++ + Tend friction rubs 0 +++ Renal crisis 0 + Centromere Ab +++ +/0 Anti-Scl 70 Ab + ++ Comparison CREST v. PSS + Relative percentages: +++++ 81-100%; ++++ 61-80%; +++ 41-60%; ++ 21-40%; + 1-20%
Treatment of Scleroderma • Localized: none • Raynauds: warmth, skin protection, vasodilator therapy • CREST: same as Raynauds • PSS: none proven • No Value: Steroids, Penicillamine, MTX • Cytoxan: for lung disease? • Experimental: stem cell transplant, TNF-I • Epoprostenol (Flolan): Prostacyclin • Bosentan (Tracleer): Endothelin receptor antagonist • Finger ulcers: difficult; vasodilators, Abx
Inflammatory Myositis: Polymyositis/Dermatomyositis • F:M = 2:1 • Acute onset • Weakness (+ myalgia): Proximal > Distal • Skeletal muscle: dysphagia, dysphonia • Sx: Rash, Raynauds, dyspnea • 65% elevated CPK, aldolase • 50% ANA (+) • 90% +EMG • 85% + muscle biopsy
Proposed Criteria for Myositis • Symmetric proximal muscle weakness • Elevated Muscle Enzymes (CPK, aldolase, AST, ALT, LDH) • Myopathic EMG abnormalities • Typical changes on muscle biopsy • Typical rash of dermatomyositis • PM Dx is Definite with 4/5 criteria and Probable with 3/5 criteria • DM Dx Definite with rash and 3/4 criteria and Probable w/ rash and 2/4 criteria
Polymyositis ClassificationBohan & Peter • Primary idiopathic dermatomyositis • Primary idiopathic polymyositis • Adult PM/DM associated with neoplasia • Childhood Dermatomyositis (or PM) • often associated with vasculitis and calcinosis • Myositis associated with collagen vascular disease
MYOPATHY: HISTORICAL CONSIDERATIONS • Age/Sex/Race • Acute vs. Insidious Onset • Distribution: Proximal vs. Distal • Pain? • Drugs/Pre-existing Conditions • Neuropathy • Systemic Features
DDX MYOPATHIIES • Toxic/Drugs • Etoh, Cocaine, Steroids, Plaquenil, Penicillamine, Colchicine, AZT, Statins, Clofibrate, Tryptophan, Taxol, Emetine • Infectious • Coxsackie, HBV, HIV, Stept, Staph, Clostridium, Toxoplasma, Trichinella • Inflammatory Myopathies • Congenital/metabolic myopathies • Neuropathic/Motor Neuron Disorders-MG, MD • Endocrine/Metabolic-hypothyroidism • Inclusion body myositis
NONMYOPATHIC CONSIDERATIONS • Fibromyalgia/Fibrositis/Myofascial Pain disorder • Polymyalgia Rheumatica • Caucasians, > 55 yrs, M=F • ESR > 100, normal strength, no synovitis • CTD (SLE, RA, SSc) • Vasculitis • Adult Still's Disease
INFLAMMATORY MYOSITISImmunopathogenesis • Infiltrates - T cells (HLA-DR+) & monocytes • Muscle fibers express class I & II MHC Ags • T cells are cytotoxic to muscle fibers • t-RNA antibodies: role? FOUND IN <50% OF PTS • Infectious etiology? Viral implicated • HLA-B8/DR3 in childhood DM • DR3 and DRW52 with t-RNA synthetase Ab
DERMATOMYOSITIS5 Skin Features • Heliotrope Rash: over eyelids • Seldom seen in adults • Gottrons Sign/Papules (pathognomonic): MCPs, PIPs, MTPs, knees, elbows • V-Neck Rash: violaceous/erythema anterior chest w/ telangiectasias • Periungual erythema, digital ulcerations • Calcinosis