IMMUNODIAGNOSTIC
IMMUNODIAGNOSTIC. Anna Tjandrawati Clinical Pathology Department Medical Faculty Padjadjaran University Dr Hasan Sadikin General Hosptital Bandung. THE COMPONENT OF IMMUNITY. INNATE/NATURAL/NON SPECIFIC IMMUNITY : Normal flora Anatomic barriers Inflammation (complement)

IMMUNODIAGNOSTIC
E N D
Presentation Transcript
IMMUNODIAGNOSTIC Anna Tjandrawati Clinical Pathology Department Medical Faculty Padjadjaran University Dr HasanSadikin General Hosptital Bandung
THE COMPONENT OF IMMUNITY • INNATE/NATURAL/NON SPECIFIC IMMUNITY: • Normal flora • Anatomic barriers • Inflammation (complement) • Phagocytic cells ADAPTIVE/ACQUIRED/SPECIFIC IMMUNITY: Lymphocytes HUMORAL: B lymphocytes Plasma cells Antibody CELLULLAR: T lymphocytescells Lymphokines
ANTIBODIES/IMMUNOGLOBULINS Proteins produced by plasma cells and secreted into body fluids in response to antigen exposure CLASSES OF IMMUNOGLOBULINS IgG:Long lasting immunity, crosses the placenta IgM:First response antibody IgA:Present in secretions IgD:Functions unknown IgE: Allergic reactions
IMMUNE RESPONSE • Secondary Antibody response/ Anamnestic response: • After reexposure to ag • Antibody production increases rapidly • IgG increase in 2 – 3 days and • increases higher levels than primary • response and remains detectable for • months or years • Primary Antibody response: • First exposure to ag • IgM appears 3-5 days, • increased and then drops • over a few weeks-months • IgG detectable 1-2 weeks , • increased and decreases • over a period of time
A Healthy immune system is fundamental to overall good health Diseases involving the immune system Immunocompetent Immunocompromised Overactive/misdirected Acquired: immunosupression drugs, microorganism Inherited: Chromosomal, gene Hypersensitivities Autoimmune disease
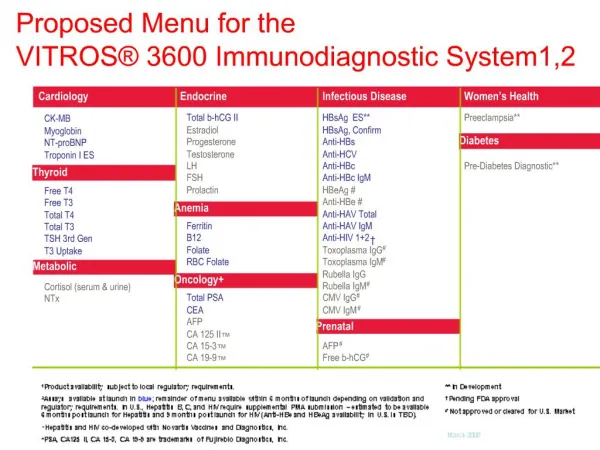
TYPES OF IMMUNOLOGICAL TESTS • Tests of immune function: • CD4, CD8 • Quantitation of Ig subgroup • Tests of leucocyte function • Allergy tests Tests based on Ag-ab reaction: The presence of an ab to a defined ag depends on the immune response of the patients Ab detection (qualitative/quantitative) is used to evaluate N or AbN immune responses
IMMUNODIAGNOSTIC Clinical Laboratory Methods for Detection of Antigens(Ag) and Antibodies(Ab) Antigen-antibody interactions underlie many immunological technique, in which the high specificity of the ab is used to identify,isolate or quantify a particular ag The technique can identify ag or ab
The classical illustration of ag-ab reaction in-vitro is THE PRECIPITIN REACTION
Antibody excess zone: The amount of Ag is insufficient to react with and precipitate all the ab present, thus free ab can be detected in the supernatant (PROZONE EFFECT) Equivalence zone: The added ag is sufficient to combine with and precipitate all the ab present and neither free ag nor ab can be detected in the supernatant Antigen excess zone: The amount of ag exceeds that required to bind all the ab and this leads to a reduction in the amount of ab precipitated. This falls is due to the formation of soluble ag-ab complex by the excess ag
Testing methods that depend on formation of immune complex Immunodiffusion Immunodiffusion (ID) is the simple technique by which ag and abs are placed in separate wells within a semisolid medium (agar) then allowed to mix through the medium by diffusion When a zone of equivalence is reached, a line ofprecipitation occurs Eg. Total Ig G, total IgM and total IgA
Precipitin reaction in gels: immuno-double diffusion-Antibody binding
Agglutination Agglutination assay that test for the presence of an ab depend on the availability of a particle that is coated with the appropriate ag. The particle can be an RBC (hemaglutination), synthetic particle (latex agglutination) and can be seen in the tube, microtitres well or simple glass slide.
The antibody is mixed with the particulate antigen and a positive test is indicated by the agglutination of the particulate antigen. Y + Y Y AGGLUTINATION test
Agglutination Latex agglutination RBC/Haemagglutination • E.g : • RA factor • Pregnancy test • CRP • ASLO E.g: * ABO Blood typing * TPHA
Latex Agglutination for Rheumatoid factor RA/ are autoantibodies, usually of the IgM class, directed agaist human IgG Principle the test: Latex particle are coated with specially treated human IgG. When serum containing RF is mixed with the IgG coated latex particle, the RF bind to the IgG and cause agglutination of the particle
ELISA(Enzyme-linked immunoassay) • The ab or ag is fixed to a surface, such as a well or • microtiter plate or plastic bead. • The test sample is applied and bound material is • detected by secondary, enzymatically labeled antibody • enzym + substrates a colored product • Spectrophotometer E.g: Anti CMV IgM, Anti Rubella IgG,Anti HAV, Anti HCV Tumor marker, Hormon
Ab/Ag + secondary enzymatically labeled antibody (conjugate) + substrate product (chromogen) .
IMMUNOCHROMATOGRAPHY • RAPID • EASY TO PERFORM • LIMITED SENSITIVITY & SPECIFICITY
15 min • Add 10µL of blood or serum • Release of Assay Reagents • IgG Capture Line • Antibody Complexing • Control Line • IgM Capture Line Assay Principle • Colloidal Gold Pad • Flavivirus specific MAb • conjugated to gold colloid • Dengue 1-4 Recombinant Antigens • Add 2 drops of running buffer • Membrane with Immobilised Antibodies • IgM capture line • IgG capture line • Control Line • Blood Separation Device • Wicking Material • Cassette Enclosure • Backing Sheet • Release of Serum Components • Absorbent Pad
Immunohistochemical methods INDIRECT Immunofluorescence Assay (IFA) The specific ag conjugated to the cells or tissues and the patient serum incubated with the cells. Unbound ab removed by washing, and the specifically bound ab are visualized with fluorescently labeled anti-Ig antisera. When observed in the fluorescence microscope againts a dark background, fluorescent labeled anti-Ig antisera bound specifically to agab complex can be visualized by their bright color E.g: ANA, anti DS-DNA
RESULT OF ANA TEST NEG. ANA POS. CONTROL NEG. CONTROL Homogenous
RESULT OF ANA TEST POS. ANA POS. CONTROL NEG. CONTROL Homogenous Homogenous
RESULT OF ANA TEST POS. ANA POS. CONTROL NEG. CONTROL Nucleolar Nucleolar