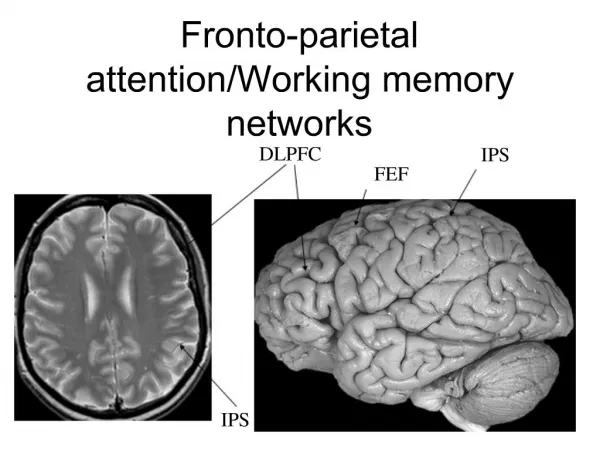
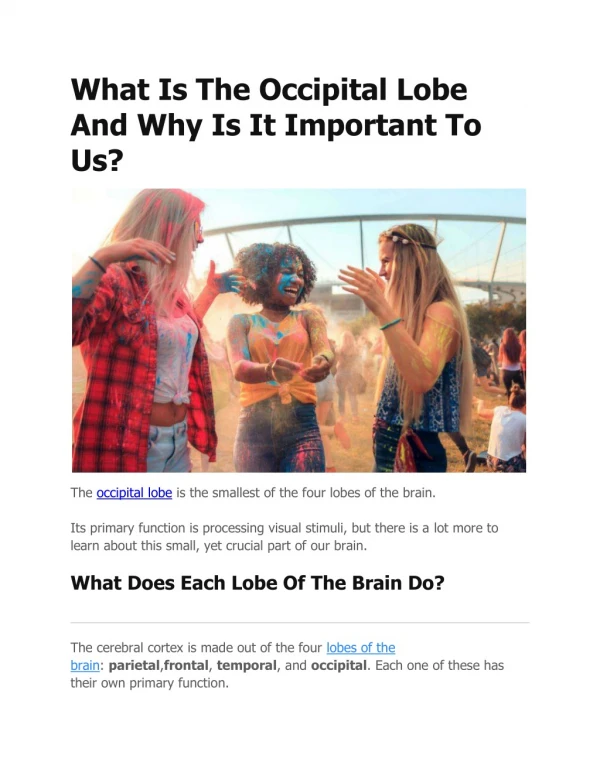
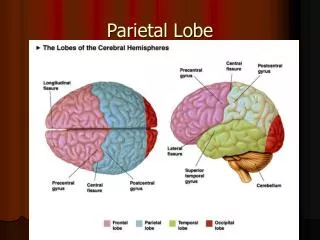
Parietal Lobe
Parietal Lobe. Superior BA 5 & 7. Superior and Inferior Aspects. Inferior BA 39 & 40. Dorsal and Ventral Streams – Where and What. Parietal Lobe Function. Somatosensory (anterior strip) Visual guidance of movements (superior)

Parietal Lobe
E N D
Presentation Transcript
Superior • BA 5 & 7 Superior and Inferior Aspects Inferior BA 39 & 40
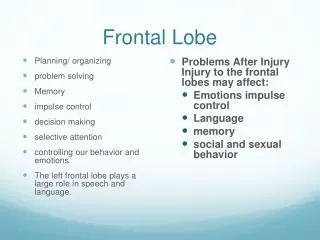
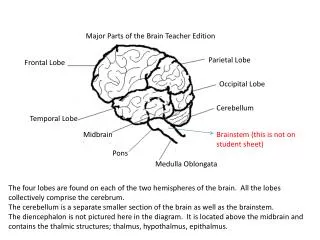
Parietal Lobe Function • Somatosensory (anterior strip) • Visual guidance of movements (superior) • Spatial cognition and quasi-spatial processes like math and reading (inferior) • Selective attention – shifting attention, disengagement, recruitment, and release (cingulate too) • Polymodal integration • Disorders of visuospatial exploration • Anosognosia (unawareness or denial of illness)
Defects of visuospatial exploration • Displace visual attention • Inability to perceive more than one stimulus (simultagnosia = simultaneous agnosia) • Defective visual control of movement (optic ataxia) • Inability to follow moving target • Inability to maintain fixation • Inability to voluntarily direct gaze to target (gaze apraxia) • Abnormal visual search
Posting performance Balint’s Normal Optic Ataxia Optic Ataxia
Characteristics of Spatial Functions: • modality-independent • visual, auditory, tactile, olfactory stimuli all have spatial location information • perception of location is an abstract concept located in a mental coordinate system • loss of spatial function affects all modalities
Category Function Brain area 1) Spatial Attention Attention to left hemispace Right parietal Attention to right hemispace Left parietal 2) Spatial Perception Object Localization R&L occipital and parietal lobes Line orientation Right parietal 3) Spatial Construction Building with blocks; R&L parietal Drawing 4) Spatial mental Mental Rotation Right parietal operations Mental Imagery “posterior”
Visual Spatial Disorders range from basic visual sensory deficits to more abstract visual spatial disability. Spatial Localization great difficulty localizing objects in two and three dimensional space. Stereopsis (binocular depth perception) is often impaired. Topographical Disorientation Errors in forming spatial maps and using them to find places or solve topographical problems Visual Spatial Construction difficulty with drawing and assembling 2D or 3D objects. Assessment Asked to draw simple figures, such as a flower, square or the face of a clock. Pencil-and-paper mazes Block design Line orientation test Visual Spatial Disorders
Finger Agnosia patients cannot identify their own fingers or those of another person. Right-Left Disorientation Lesions of the left parietal lobe commonly result in right-left disorientation. Assessment AutopagnosiaHave patient point to own body parts and those on others Finger AgnosiaHave patient close their eyes and indicate which of their fingers has just been touched. Body Schema Disturbance
Newberg et al (2001) • Used SPECT neuroimaging to scan eight experience Tibetan Buddhist meditators. Increased activation Decreased activation
Blanke et al (2002) • Stimulation of the right angular gyrus caused reliable out of body experiences. • Further evidence for the role of the parietal cortex in meditating self - other boundaries.
Neglect Syndrome (a.k.a Hemi-neglect) • Fails to respond to meaningful stimuli presented to side opposite brain lesion (contralateral space) • Ignores people on one side of room; eats from only one side of plate; draws half of an object, grooms half their body. • But can adapt by learning to turn plate; to turn head; to move objects across visual field. • Not due to motor defects • Occurs in • 30-90% Right hemisphere damaged patients (RHD), depending on type of patient (tumor, injury, etc) and type of test • 2-15% Left hemisphere damage (LHD) Right Parietal Stroke – recovery at 2 months, 4 months, 6 months, 9 months
Line Bisection Test • (similar to item cancellation, every “e”)
Pseudo-neglect • Which appears darker?
Pseudo-neglect • Which appears darker? • Normals overattend to the LVF?
Neglect according to Kinsbourne’s hypothesis • Hemispheres normally compete for attentional control. • With damage, intact hemisphere dominates. • A release sign or positive symptom: left neglect involves “over attending” to the right.
Evidence of implicit recognition • House on fire example • Which house do you prefer? • Unconscious perception of left side of space
Apraxia • Difficulty in sequencing & executing movements
Characterized by movement of the wrong part of the limb incorrect movement of the correct part, or correct movements but in the incorrect sequence. Often assessed by requesting patient to demonstrate the use of a tool or household implement (e.g., "Show me how to cut with scissors"). Limb Apraxia
Buccofacial Apraxia • Difficulty performing skilled movements with lips, face, tongue, larynx, and pharynx. • E.g., when asked to blow out a match, suck on a straw or blow a kiss, s/he unable to make the movements or makes uncoordinated movements. • S/he may substitute incorrect movements or perseverate, or substitute verbal expressions for the movement. (e.g., when asked to blow out a match, the patient might say "Blow“).
Normal scan path Gaze apraxic scan path
Gaze apraxia Back and forth between two points normal Outlining the Perimeter of a rectangle normal
Patient with constructional apraxia due to lesion of the right parietal lobe.
Ideational Apraxia • Cannot perform a series of acts although able to perform individual components of the series. May correctly perform each step (say, in making coffee but out of order, such as turning coffee maker on first). • Loss of conceptual knowledge associated with objects and overall goal of the activity sequence. • not localized, often observed in dementia.