Download
1 / 48
520 likes | 749 Vues
This comprehensive guide explores anatomy, diseases, and clinical cases related to benign thyroid disorders, with a focus on surgical management. Learn about risk factors, diagnostic guidelines, and treatment options in thyroid surgery.

E N D
Surgical management of benign thyroid disorders Nidal Younes MD Professor of Endocrine Surgery and Diabetic Foot Consultant- Jordan University Hospital
A light in the dark middle ages in Europe At-Tasrif liman 'Ajiza 'an at-Ta'lif (The Method of Medicine). At-Tasrif is a medical encyclopaedia compendium of 30 volumes compiled from medical data that Al-Zahrawi accumulated in a medical career that spanned five decades of teaching and medical practicewithout doubt Albucasis was the chief of all surgeons“ Pietro Argallata Albucasisابو القاسم الزهراوي
Emil Theodor Kocher • 1841 – 1917 • 1909 Nobel prize in medicine “physiology, pathology, surgery of thyroid” • promotion of aseptic surgery and scientific methods in surgery. • reducing the mortality of thyroidectomy to less than 1%
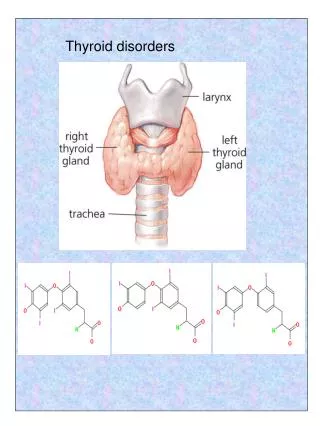
Thyroid Hormone Synthesis • Iodide trapping • Oxidation of iodide and iodination of thyroglobulin • Coupling of iodotyrosine molecules within thyroglobulin (formation of T3 and T4) • Proteolysis of thyroglobulin • Deiodination of iodotyrosines • Intrathyroidal deiodination of T4 to T3
Effects of Thyroid Hormone • Fetal brain and skeletal maturation • Increase in basal metabolic rate • Inotropic and chronotropic effects on heart • Increases sensitivity to catecholamines • Stimulates gut motility • Increase bone turnover • Increase in serum glucose, decrease in serum cholesterol
Benign Thyroid Disease • Benign Nontoxic Conditions • Diffuse and Nodular Goiter • Benign Toxic Conditions • Toxic Multinodular Goiter • Graves’ Disease • Toxic Adenoma • Inflammatory Conditions • Chronic (Hashimoto’s) Thyroiditis • Subacute (De Quervain’s) Thyroiditis • Riedel’s Thyroiditis
Goiter enlargement of the thyroid gland (local or diffuse) based on hyperplasia or degeneration
Classification • Benign Nontoxic Conditions • Diffuse and Nodular Goiter • Benign Toxic Conditions • Toxic Multinodular Goiter • Graves’ Disease • Toxic Adenoma
Diffuse nontoxic goiter • Iodine deficiency results in hypothyroidism • Increasing TSH causes hypertrophy of thyroid
Multinodular goiter • Follicles may become autonomous; certain follicles will have greater intrinsic growth and functional capability
Toxic multinodular goiter • Follicles continue to grow and function despite decreasing TSH
Clinical case • 52 y.o. female with no active medical problems. During routine physical, note a thyroid nodule. Told by a surgeon last year not to worry about it. • PE: 1 x 2cm R lower pole nodule. What information do you want from the patient?
Age as a Risk Factor • Age • young patients (<20 years of age) thyroid nodules are much more likely to be malignant (40-50%). • elderly (>60 years of age) -higher risk, especially of more aggressive thyroid tumors.
Gender and Thyroid Nodules • Gender • male -higher risk if nodule present • females • have many more nodules • less likely to be malignant. • still have majority of thyroid cancers
Other major risks • Radiation to head and neck. • 40% risk of thyroid cancer usually 25 years later. • Children with Hodgkin's lymphoma • Family History of MEN II, Gardner’s Syndrome, Cowden’s disease.
Red Flags • Recent growth • Soft tissue swelling • Vocal changes • Dysphagia • Signs of thyroid dysfunction
Clinical case • 26 y.o. female with a 2-3 year history of goiter. No symptoms. • P.E.: 3x4 cm Right sided thyroid mass, firm, adherent to soft tissue. What physical findings are worrisome? How can you best clarify the nature of the nodule?
Diagnostic guidelinesATA 2009 • Measure serum TSH in the initial evaluation of a patient with a thyroid nodule. If the serum TSH is subnormal, a radionuclide thyroid scan should be performed using either technetium 99mTc pertechnetate or 123I. Recommendation rating: A • Thyroid sonography should be performed in all patients with known or suspected thyroid nodules. Recommendation rating: A • FNA is the procedure of choice in the evaluation of thyroid nodules. Recommendation rating: A • US guidance for FNA is recommended for those nodules that are nonpalpable, predominantly cystic, or located posteriorly in the thyroid lobe. Recommendation rating: B
ATA Thyroid Nodules and Cancer Guidelines 2015 • Differences between the 2009 and 2015 • 2009 2015 • Recommendations 80 101 • Sub-recommendations 103 175 • References 437 998 • Tables 5 17 • Figures 5 8
Examples of Grading changes • 2009 Recommendation: Measure serum TSH during the initial evaluation of a patient with a thyroid nodule. (Recommendation A) • 2015 Recommendation: Measure serum TSH during the initial evaluation of a patient with a thyroid nodule. (Strong recommendation, Moderate-quality evidence)
Thyroid Ultrasound • Can identify presence of nodules. • May be able to characterize follicular vs. solid. • Not able to rule our malignant nodule • Aid in biopsy. Thyroid
Sonographic patterns • High suspicion [malignancy risk 70-90%]: Solid hypoechoic nodule or solid hypoechoic component of a partially cystic nodule with one or more of the following features: irregular margins, microcalcifications, taller than wide shape. • Intermediate suspicion [malignancy risk 10-20%]: Hypoechoic solid nodule without high suspicion features • Low suspicion [malignancy risk 5-10%]: Isoechoic or hyperechoic solid nodule, or partially (> 50%) cystic nodule, with eccentric solid area without high suspicion features • Very low suspicion • Benign purely cystic
Fine-Needle Aspiration • Best tool for determining pathology other than surgical excision. • Can be as high as 80 % sensitive and 95% specific. • Operator dependent in obtaining adequate amount of tissue. 25 gauge needle is optimal. • Should not be relied on if negative in patient with previous neck irradiation. • Multifocal tumors common.
FNA Recommendations (8) • Recommendations for diagnostic FNA based on sonographic features: • Nodules > 1 cm with high suspicion sonographic pattern (Strong recommendation, Moderate-quality evidence) • B) Nodules > 1cm with intermediate suspicion sonographic pattern (Strong recommendation, Low-quality evidence) • C) Nodules > 1.5 cm with low suspicion sonographic pattern (Weak recommendation, Low-quality evidence) • D) Nodules > 2 cm with very low suspicion sonographic pattern (e.g. - spongiform) (Weak recommendation, Moderate-quality evidence
Interpreting the Biopsy Report • What you get: • benign • indeterminate • Suspicious/ malignant • inadequate specimen • What it means: • benign - 90-95% likelihood it is benign • indeterminate- who knows? • suspicious- it’s malignant. • inadequate specimen - do it again (and again)
Treatment of Diffuse or Multinodular Goiter • Observation • I-131 • Surgical Therapy • Total thyroidectomy • Subtotal thyroidectomy • Hemithyroidectomy
Graves’ Disease • Most common form of thyrotoxicosis • Autoimmune etiology with familial predisposition • Thyroid receptor stimulating antibody unique to Graves’ disease; other autoantibodies present (TgAb, TPOAb) • Affects females five times more often than males
Presentation of Graves’ Disease • Thyrotoxicosis: palpitations, nervousness, easy fatigability, diarrhea, excessive sweating, intolerance to heat, weight loss • Eye signs • Diffuse goiter
Diagnosis of GD • A radioactive iodine uptake should be performed when the clinical presentation of thyrotoxicosis is not diagnostic of GD; a thyroid scan should be added in the presence of thyroid nodularity. 1/+00
Treatment • Antithyroid Drugs • May require prolonged therapy • Radioactive iodine • May worsen ophthalmopathy unless followed by steroids • Surgery • Make patient euthyroid prior to surgery • Potassium iodide two weeks prior to surgery can decrease the vascularity of the gland
ATA guidelines 2011 • RECOMMENDATION 22Whenever possible, patients with GD undergoing thyroidectomy should be rendered euthyroid with methimazole. Potassium iodide should be given in the immediate preoperative period. 1/+00
Thyroid Storm • Thyroid storm: manage aggressively with beta-blockers, calcium channel blockers, PTU, methimazole, sodium iodide, digitalis or diuretics for heart failure, fluid and electrolyte management
Toxic Adenoma • Autonomously functioning thyroid nodule hypersecreting T3 and T4 resulting in thyrotoxicosis (Plummer’s disease) • Almost never malignant • Rx with antithyroid drugs followed by either I-131 or surgery
Chronic Thyroiditis • Also known as Hashimoto’s disease • Probably the most common cause of hypothyroidism in United States • Autoantibodies include: thyroglobulin antibody, thyroid peroxidase antibody, TSH receptor blocking antibody
Pathology of Chronic Thyroiditis • A dense infiltrate of plasma cells and lymphocytes with germinal center formation is seen in this thyroid. Cells of the individual colloid follicles often display abundant pink granular cytoplasm, which is referred to as oncocytic change, in this setting. These cells are referred to as Hurthle cells or oncocytes - these are metaplastic.
Presentation and Course • Painless goiter in a patient who is either euthyroid or mildly hypothyroid • Low incidence of permanent hypothyroidism • May have periods of thyrotoxicosis • Treat with levothyroxine
Subacute ThyroiditisDe Quervain's thyroiditis • Most common cause of thyroid pain and tenderness • Acute inflammatory disease most likely due to viral infection • Transient hyperthyroidism followed by transient hypothyroidism; permanent hypothyroidism or relapses are uncommon • Inflammation of thyroid gland that includes granulomas • Painful swallowing (odynophagia), sore throat, thyroid region tenderness, fever, fatigue, malaise
Treatment of Subacute Thyroiditis • Symptomatic: NSAIDS or a glucocorticoid • Beta-blockers indicated if there are signs of thyrotoxicosis • Levothyroxine may be given during hypothyroid phase
Riedel’s Thyroiditis • Rare disorder usually affecting middle-aged women • Likely autoimmune etiology • Fibrous tissue replaces thyroid gland • Patients present with a rapidly enlarging hard neck mass