Download
1 / 7
100 likes | 270 Vues
Canadian Diabetes Association Clinical Practice Guidelines Management of Stroke in Diabetes. Chapter 27 Michael Sharma, Gord Gubitz. Stroke in Diabetes Checklist. 2013. SCREEN for diabetes in all patients admitted with ischemic stroke or Transient I schemic A ttack (TIA)

E N D
Canadian Diabetes Association Clinical Practice GuidelinesManagement of Stroke in Diabetes Chapter 27 Michael Sharma, GordGubitz
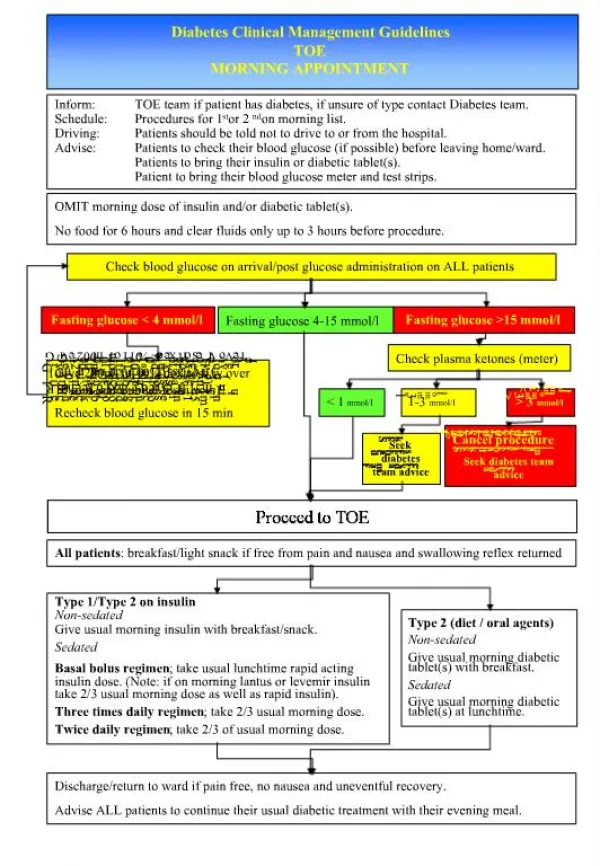
Stroke in Diabetes Checklist 2013 • SCREEN for diabetes in all patients admitted with ischemic stroke or Transient Ischemic Attack (TIA) • MANAGE in-hospital glycemia as one would for any other reason for admission • TREAT the ischemic stroke or TIA in a patient with diabetes the same as a patient without diabetes, using Canadian Stroke Strategy Best Practices Recommendation http://www.strokebestpractices.ca
Patients with DM are 2-3X More Likely to Have a Stroke Public Health Agency of Canada (August 2011); using 2008/09 data from the Canadian Chronic Disease Surveillance System (Public Health Agency of Canada).
People with Diabetes and Stroke Have Worse Outcomes • Increased hospital and long-term mortality • More residual neurologic disability • More residual functional disability • Longer hospital stays Idris I, et al. Int J ClinPract 2006;60:48-56.
Treat Glycemia the Same as in Other Conditions • Usually premeal BG 5-8 mmol/L, random <10 mmol/L • Cochrane Systematic Review of 7 randomized controlled trials of intensive insulin therapy (target BG 4-7.5 mmol/L) versus usual care in acute ischemic stroke showed no benefit in the outcomes of death, disability or dependence, and there was an increase in hypoglycemia Bellolio MF, et al. Cochrane Database of Systematic Reviews 2011Sep 7;(9):CD005346.doi:10.1002/13651858.CD005346.pub3.
Recommendations 1 and 2 2013 • Patients with ischemic stroke or transient ischemic attack should be screened for diabetes with a fasting plasma glucose, A1C, or 75-g OGTT soon after admission to hospital [Grade D, Consensus] • All patients with diabetes and ischemic stroke or transient ischemic attack (TIA) should receive the same treatments that are recommended for patients with ischemic stroke or TIA without diabetes since they benefit equally[Grade D, Consensus]
CDA Clinical Practice Guidelines http://guidelines.diabetes.ca – for professionals 1-800-BANTING (226-8464) http://diabetes.ca – for patients