Download
1 / 11
110 likes | 209 Vues
Alliance for Health Reform Inside Deficit Reduction: What it Means for Medicare Tricia Neuman Senior Vice President and Executive Director, Program on Medicare Policy Kaiser Family Foundation October 11, 2011. Medicare and Deficit Reduction. Premium Support/Defined Contribution.

E N D
Alliance for Health Reform Inside Deficit Reduction: What it Means for Medicare Tricia Neuman Senior Vice President and Executive Director, Program on Medicare Policy Kaiser Family Foundation October 11, 2011 Medicare and Deficit Reduction
Premium Support/Defined Contribution • Proposals would transform Medicare from a defined benefit program to a defined contribution or premium support plan • Proposals vary in how government contributions would be determined and indexed, which benefits would be covered, the role of traditional Medicare, treatment of low income, etc. • Bowles-Simpson suggested premium support as an option to consider, if costs grow faster than federal health spending targets (Nov. 2010) • Domenici-Rivlin endorsed premium support, with traditional Medicare as a default option (Dec. 2010) • Rep. Paul Ryan proposed a defined contribution system, beginning in 2022; also reflected in the House Concurrent Budget Resolution (April 2011)
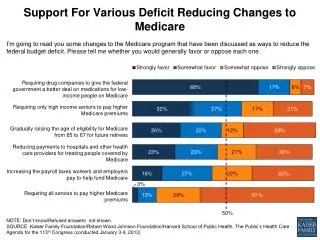
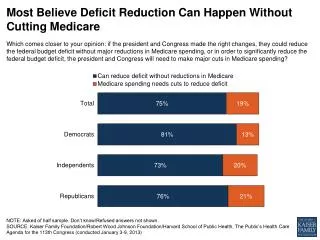
Raising the Age of Medicare Eligibility to 67 • Proposal has been raised as an option to reduce Medicare spending, reflecting view that beneficiaries live longer than in 1965 • Bowles-Simpson suggested raising the eligibility age as option to consider if federal health spending exceeds targets (November 2010) • Numerous studies have documented potential for large increase in uninsured 65 and 66 year olds if without Medicare – pre ACA • With fully implemented health reform law, 65 and 66 year olds should be able to gain coverage through Medicaid or the exchange, or an employer if they choose to work longer • Medicare achieves savings, but savings would be partially offset by new costs of coverage for 65 and 66 year olds in the exchange and Medicaid • Costs would be shifted to other Medicare beneficiaries (higher Part B premiums), individuals in the exchanges (higher insurance premiums), employers and Medicaid • CBO (March 2011) projects federal savings of $124.8 (2012-2021) assuming gradual phase in beginning in 2014 of 2 months per year
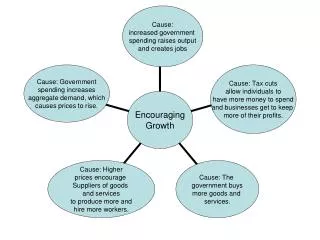
Raising Medicare Age of Eligibility to 67Analysis assumes implementation of higher age and health reform in 2014 Winners and Losers Effect on Total Health Costs No change in out-of-pocket spending 3% 66% would pay MORE out of pocket 31% would pay LESS out of pocket Total Number of Full-Year Equivalent Medicare Beneficiaries Affected = 5.0 million SOURCE: Kaiser Family Foundation, “Raising the Age of Medicare eligibility: A Fresh Look Following Implementation of Health Reform,” July 2011.
Restructuring Medicare Cost Sharing Requirements • Recent proposals would restructure Medicare cost-sharing requirements to achieve savings • Restructuring could also simplify the program, provide greater financial protections, and mitigate the need for supplemental insurance • Bowles-Simpson and Domenici-Rivlin propose combining the Part A and B deductibles (~$550), adding 20% coinsurance for all services (inpatient hospital, home health, etc.), and new limit on out-of-pocket spending • Federal savings expected due to new coinsurance requirements (for some) and higher deductible (for many) • Out-of-pocket spending expected to decrease for small share, but increase for the majority who use relatively few services • CBO estimates similar proposal would save $32.2 billion, 2012-2021 • President’s plan would allow IPAB to consider value-based benefit designs
Medigap: Prohibiting “First Dollar” Coverage • Proposals would prohibit/discourage first dollar Medigap coverage, giving beneficiaries with Medigap more “skin in the game” • Exposing beneficiaries to higher cost-sharing services would be expected to reduce their utilization of Medicare-covered; as utilization of services declines, Medicare spending would decrease and as a result, Medigap premiums should decrease • Bowles-Simpson would prohibit Medigap from covering first $500 of cost sharing and limit coverage to 50% of next $5,000 • CBO (March 2011) estimates savings of $53.4 billion over 10 years • Would affect all beneficiaries with first-dollar Medigap. Today, more than 8 million Medicare beneficiaries have a Medigap policy, most of whom have first-dollar coverage • President’s plan would impose 30% Part B premium surcharge on new enrollees who purchase first dollar Medigap policies, beginning in 2017 • OMB (Sept 2011) estimates $2.5 billion in savings over 10 years • Would not apply to current beneficiaries
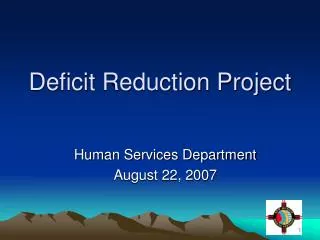
Share of Medicare Beneficiaries with Medigap First Dollar Coverage, 2010 EXHIBIT 6 National Average = 12% 0%-5% (5 states, DC) 6% - 10% (13 states) 11% -15% (16 states) 16% - 20% (8 states) 21% - 30% (2 states) More than 30% (5 states) SOURCE: K. Desmond, T. Rice, and Kaiser Family Foundation analysis of 2010 National Association of Insurance Commissioners (NAIC) Medicare Supplement data.
Increase Medicare Premiums • Domenici-Rivlin would increase beneficiaries’ Part B premiums to cover 35% of program costs (up from 25%) • $241.2 billion in savings over 10 years (CBO) • President’s plan would modify Medicare Part B and D income-related premiums • Under current law, individuals with incomes above $85,000, or couples with incomes above $170,000 pay a larger share of Part B and D premiums; income levels are frozen through 2019 • Proposal would continue to freeze income-related premium thresholds beyond 2019 until 25% of beneficiaries pay the income-related premium, and would increase premium contributions by 15%, beginning in 2017 • $20.0 billion in savings over 10 years (OMB)
Income Distribution of the Medicare Population, 2010 Less than 1%had incomes above $150,000 5%had incomes above $87,023 50% had incomes below $21,183 25% had incomes below $12,760 NOTE: Total household income for couples is split equally between husbands and wives to estimate income for married beneficiaries. SOURCE: Urban Institute / Kaiser Family Foundation analysis, 2011.
Independent Payment Advisory Board (IPAB) • The IPAB, established under the health reform law, is required to make Medicare savings recommendations if Medicare growth rates exceed specified target growth rates • Secretary of HHS must implement IPAB recommendations or an alternative enacted by Congress • CBO originally (March 2010) estimated savings of $15.5 billion from 2015-2019; in June 2011, CBO updated estimate assumes no savings attributable to IPAB during the 10-year budget window ending 2020 • Proposals to modify IPAB • President’s plan would lower the target growth rate from per capita GDP +1% to GDP+0.5% beginning in 2018; IPAB would make recommendations to promote “value-based benefit design” • Bowles-Simpson would allow IPAB to make recommendations for all providers (no exceptions); if costs grow faster than targets, could consider changes to cost sharing and benefits and look beyond Medicare for savings • Domenici-Rivlin would require IPAB to review Medicare benefit structure every 2 years and recommend conforming changes to private market (to become law unless blocked by Congress) • Rep. Roe (and others) – repeal IPAB (CBO says this would COST $2.4 billion from 2018-2021)
Other Medicare Proposals • Apply Medicaid drug rebate for Part D LIS recipients • Proposed by Bowles-Simpson and the President ($135 billion over 10 years, OMB) • Impose cap on federal health/Medicare spending • Bowles-Simpson would set global target for total federal health spending at GDP+1 percent, with potential saving proposals if spending exceeds target • Domenici-Rivlin would limit federal support per Medicare enrollee to GDP+1% per capita • Give Medicaid full responsibility for the health coverage Medicare beneficiaries also eligible for Medicaid (dual eligibles) and mandate their enrollment in Medicaid managed care plans (Bowles-Simpson) • Home Health Copayments • $100 home health copay per episode for new enrollees (if unrelated to hospitalization), beginning 2017 ($0.4 billion over 10 years, OMB) • 10% coinsurance on all home health episodes ($40.1 billion over 10 years, CBO) • Impose additional cost sharing: • Coinsurance on first 20 days of SNF ($21.3 billion over 10, CBO) • Increase Part B deductible for new enrollees, 2017 ($1.0 billion over 10 years, OMB) • Reduce payments to providers and/or plans • Implement new delivery system reforms and quality improvements