Download
1 / 20
210 likes | 443 Vues
Medical Home Model of Care. April 23, 2010. Tupelo Group, LLC. Randy Messier, MT, MSA. Presentation Agenda. Quick Overview of our Story in Vermont Outline of Medical Home Program Medical Home Design Community Health Team (CHT) Panel Management Behavioral Health

E N D
Medical Home Model of Care April 23, 2010 Tupelo Group, LLC Randy Messier, MT, MSA
Presentation Agenda Quick Overview of our Story in Vermont Outline of Medical Home Program Medical Home Design Community Health Team (CHT) Panel Management Behavioral Health NCQA Medical Home Certification Lessons Learned
Healthcare Reform In Vermont • Blueprint for Health (2006 – 2008) • Focus: Chronic Care Model/Clinical Microsystems • 6 Pilot Communities Received Grants • Launched Statewide Collaboratives w/ 50+ practices • Blueprint for Health (2009 – 2010) • Focus: Integrated Medical Home Model • 3 of the 6 Pilot Communities Received Grants • Launched Statewide Medical Home Readiness Collaborative w/ 22+ practices
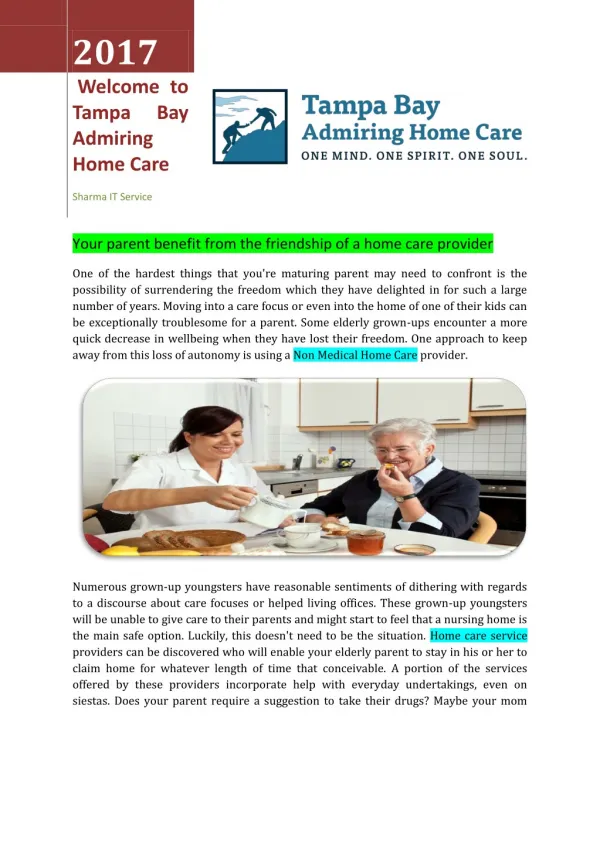
Medical Home Definition Health care setting that facilitates partnerships between individual patients, their personal physicians, and their family. Care is facilitated by: registries, information technology, health information exchange Care is delivered when and where needed. Care is delivered in a culturally and linguistically appropriate manner.
Global Aim Statement We aim to improve care to our patients by implementing a patient centered medical home. The process begins with identifying and evaluating our patients and their current health status and ends with improved outcomes. By working on this process we expect to: Improve quality Engage and empower patients Educate, and foster a team approach to care management Improve efficiency within the practice It is important to do this now because the 1:1 visit alone leaves Primary Care unsustainable.
FAHC Jeffords Institute for Clinical and Operational Effectiveness
FAHC Jeffords Institute for Clinical and Operational Effectiveness
Community Health Team (CHT) Services include: • Nutrition help • Exercise advice • Diabetes Education • Medication Management • Behavioral/Mental Health • Connection to community and financial resources Providers involved in pilot can refer their patients to the CCT. Team members provide regular ongoing support as needed via phone or in person. The team helps patients set realistic goals and timelines for improving health. FAHC Jeffords Institute for Clinical and Operational Effectiveness
Panel Management MD’s determine criteria for screening patient panel. i.e. HBA1C value, HBA1C on time, Colonoscopy, mammography, PHQ9 Scores etc. Panel MA runs report, and based on predetermined algorithm designed by the providers, takes action on report. All patients who fall outside of algorithm are reviewed directly with provider.
Panel Management Searchable database is imperative to success. Predetermined algorithm and query design standardizes the process for everyone. This standard approach systematizes the preventive care component of panel management. Freeing up MD’s to be MD’s. FAHC Jeffords Institute for Clinical and Operational Effectiveness
Integrated Behavioral Health On site LICSW . Provides immediate consultation. Is a full member of the clinical team. Works with CHT on follow up and referral made via EHR. (Makes referral and tracks) Patients “DO” come back for visits. (No Show rate 5.9%) Short term intervention and support. Screening/Brief Intervention/Referral Complicated long term referred out. FAHC Jeffords Institute for Clinical and Operational Effectiveness
Medical Home Designationand Financing Agreement with payors was to become NCQA certified as a patient centered medical home. Payment directly linked to score achieved on NCQA review. Success requires financial reform. NCQA Standard update coming
NCQA Medical Home Criteria Access & Communication Patient Tracking & Registry Functions Care Management Patient Self-Management Support Electronic Prescribing Test Tracking Referral Tracking Performance Reporting & Improvement Advanced Electronic Communication FAHC Jeffords Institute for Clinical and Operational Effectiveness
PPC-PCMH Content and Scoring **Must Pass Elements
PPC 7: Referral Tracking • Element A: Referral tracking- Outside of paper medical records and patient visits, the practice uses a paper based or electronic system to assist tracking practitioner referrals designated as critical until the specialist or consultant report returns to the practice: (must pass)(4 points) • 100% - Practice uses system that includes all 4 items • 75% - Practice uses system that includes 2-3 items • 50% - Practice uses system that includes 1 item • 25% - No scoring option • 0% - System does not include any of the items • Must track referral origin, clinical detail, status and administrative detail • Paper based logs or electronic reports FAHC Jeffords Institute for Clinical and Operational Effectiveness
What We’ve Learned So Far Patients love it!! They love the extra time they have with the team. Challenged to have quick outcomes. Behavioral Health integration is essential. It’s a lot of work to get started! Not all Providers embrace systems change at the same rate. FAHC Jeffords Institute for Clinical and Operational Effectiveness
Significant Findings! • Six month follow-up data after “graduation” • Diabetes patients engaged in CHT • 59% of patients with a baseline HbA1c greater then 7 lowered their HbA1c to below 7 at follow up • 100% of patients with a baseline depression score of moderate or severe depression lowered their score to mild/not clinically significant • 100% of patients with a baseline anxiety score of moderate or severe anxiety lowered their score to mild anxiety at follow up FAHC Jeffords Institute for Clinical and Operational Effectiveness
Significant Findings! • Six month follow-up data after “graduation” • Behavioral Health referrals • 75% of patients with a baseline depression score of moderate to severe lowered their score to mild/not clinically significant at follow up. • 70% of patients with a baseline anxiety score of moderate or severe anxiety lowered their score to mild/not clinically significant at follow up. FAHC Jeffords Institute for Clinical and Operational Effectiveness