Download
1 / 22
220 likes | 281 Vues
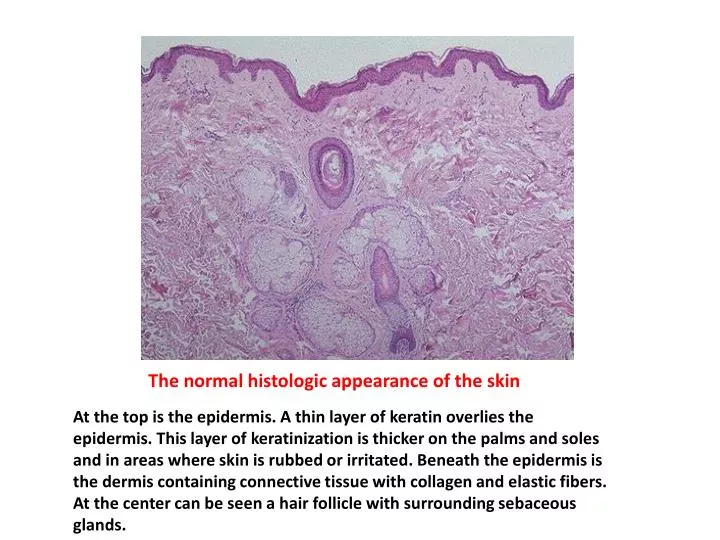
The normal histologic appearance of the skin.

E N D
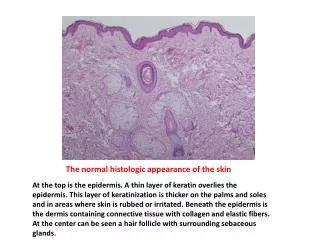
The normal histologic appearance of the skin At the top is the epidermis. A thin layer of keratin overlies the epidermis. This layer of keratinization is thicker on the palms and soles and in areas where skin is rubbed or irritated. Beneath the epidermis is the dermis containing connective tissue with collagen and elastic fibers. At the center can be seen a hair follicle with surrounding sebaceous glands.
Here are normal adnexal structures of the skin. A hair follicle is seen at the center, with sebaceous glands above and sweat glands and ducts near the base of the hair follicle.
This is psoriasis. The thick, silvery, scaling lesions are most often found over bony prominences, scalp, genitalia, and hands. It occurs when there is abnormal proliferation and turnover of epidermis (reduced from a month to only 4 days for a cell to transit from basal layer to surface).
Microscopically, psoriasis is characterized by downward elongation of the rete ridges with thinning of overlying stratum granulosum, with parakeratosis above this. Small aggregates of neutrophils with surrounding spongiform change are seen in the superficial epidermis. Capillaries within dermal papillae are brought close to the surface.
Clinical appearance of lichen planus affecting the dorsum of the hand. One of the lesions has been biopsied.
Biopsy of lichen planus showing hyperkeratosis and infiltrate that hugs irregularly acanthotic epidermis
Clinical appearance of bullous pemphigoid. Large bullae are present, some of which have ruptured.
Pemphigus vulgaris in which characteristic suprabasal bulla and dark acantholytic cells can be seen.
Pemphigus foliaceus with its high intraepidermal cleavage plane
seborrheic keratosis (SK) a very common lesion of older adults. SK's are common over the face, neck, and upper trunk. They are rough-surfaced and brown coin-like plaques that vary from a few millimeters in size to several centimeters.
This is the microscopic appearance of a seborrheic keratosis (SK). Broad bands of normal-appearing epidermal cells have large keratin-filled "horn cysts" within them.
BCC The cells of a basal cell carcinoma are dark blue and oblong with scant cytoplasm. They resemble the cells along the basal layer of normal epidermis.
Basal cell carcinoma of the skin Nests of basaloid cells are dropping off into the upper dermis. These neoplasms can be multifocal. They are slow growing . The problems they cause are related to local invasion. Metastases are quite rare.
squamous cell carcinoma arising on the dorsum of the hand. Besides sun exposure, risk factors for squamous cell carcinoma arising in skin include carcinogens such as tars, chronic ulcers, burn scars, arsenic poisoning, and radiation exposure. In this case there was a history of both sun exposure as well as exposure to carcinogens.
squamous cell carcinoma is seen at medium power Note the pleomorphism of the cells. A "squamous eddy" is seen at the upper left, but some of the cells at the right show little keratinization.
Melanocytic nevus Small brown flat to slightly raised nevi are quite common in Caucasians. They are usually less than a centimeter in diameter.
Intradermal nevus the benign nature of the nevus cells are seen below the epidermis. The cells are small and round and blue melanocytes that are in aggregates or sheets.
junctional nevus there are nevus cells in nests in the lower epidermis as well as nests appearing to "drop off" into the upper dermis. Unlike a melanoma, there is no significant atypia and no inflammation.
malignant melanoma of the skin The lesion is larger than a centimeter, has irregular borders, and irregular pigmentation, with one very dark area on the left. The prognosis of a melanoma correlates best with the depth of invasion. Sun exposure in light-skinned persons leads to melanoma formation.
microscopic appearance of melanoma Large polygonal cells (or spindle cells in some cases) have very pleomorphic nuclei with prominent nucleoli. The neoplasm is making brown melanin pigment. A Fontana-Masson stain for melanin may help to detect small amounts of cytoplasmic melanin.
A Fontana-Masson silver stain (melanin stain) will demonstrate a fine dusting of melanin pigment within the cytoplasm of the neoplastic cells of this malignant melanoma.
The neoplastic cells shown here stain positively with HMB-45, suggesting that the primary neoplasm is a melanoma