Polymyalgia Rheumatica
Polymyalgia Rheumatica. AM Report Cat Hathaway 3/16/2010. What is it?. Proximal myalgia of the hip and shoulder girdles associated with morning stiffness (at least 1 hour) Etiology is largely unknown Associated with HLA-DR4 Associated with viral infection?

Polymyalgia Rheumatica
E N D
Presentation Transcript
PolymyalgiaRheumatica AM Report Cat Hathaway 3/16/2010
What is it? • Proximal myalgia of the hip and shoulder girdles associated with morning stiffness (at least 1 hour) • Etiology is largely unknown • Associated with HLA-DR4 • Associated with viral infection? • viral infection resulting in monocyte activation • Some series show higher prevalence of antibodies to Adenovirus and RSV
Epidemiology • Elderly patients, >50 years of age • Incidence 52.5/100000 • Prevalence 0.5-0.7% • Females 2:1 • White, european (highest rates in Northern Europe) • Some evidence of genetic susceptibility • 50% Temporal arteritis patients will have PMR (15% of PMR patients will develop TA)
Clinical Picture • Often previously healthy, >50 • Bilateral proximal muscle pain and stiffness • ESR >40, CRP elevation • Prompt response to steroids • Low grade fevers, weight loss • Malaise, fatigue, depression • Difficulty getting out of bed, rising from sitting, performing ADLs • Rarely can have high spiking fevers
Exam findings • Low grade temp • Can have LE swelling • Muscle strength is NORMAL • Pain specifically in shoulder and hip girdle despite lack of clinically significant swelling • Tenderness to palpation and diminished ROM in shoulders and hips • Can get a transient synovitis (usually knee, wrist, sternoclavicular joints)
Treatment • Rule out infectious/autoimmune process • Endocarditis • RA • Lupus • Systemic Infection • Myositis • Low dose prednisone (10-15mg/d) for 2-4 weeks. Then can start trying to taper. • Vitamin D/Calcium • Steroid sparing agents (MTX, azathioprine) • NSAIDs
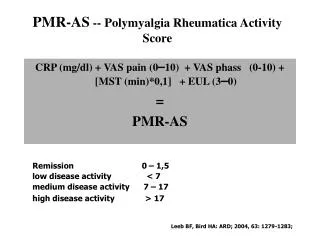
Few points about steroid therapy • Starting >10mg fewer relapses, shorter treatment periods than compared to <10mg • Starting >15mg lead to higher cumulative doses and more steroid adverse affects • Tapering lead to more successful treatment, fewer relapses, when done slowly (1mg/mo)
Prognosis • Overall, benign disease • Self limited and most resolve within 1-3 years, however patients experience significant decrease in quality of life • 50-75% of patients can often be weaned off all steroids by 3 years • If relapse, often occurs within 12 months of weaning steroids • Need to be monitored for TA
Other differentials to consider • Amyloidosis (inflammatory) • Fibromyalgia • Osteoarthritis • Shoulder disorders • Cervical spondylosis • Parkinson’s Disease • Multiple Myeloma
Tests to order • ESR (typically >40, sometimes >100), CRP • ANA, RF, Blood cultures • CBC • CK NORMAL! • Serum IL6 (not necessary, but will be elevated and often parallels disease course) • No imaging necessary but Xrays should not show erosive disease or osteopenia. • MRI if done will often show bursitis and senovitis. • TA biopsy only done if you suspect TA
Temporal Arteritis • Visual loss • Headache • Scalp tenderness • Jaw claudication • CVA • Aortic arch syndrome • Thoracic aorta aneurysm • Dissection
Bibliography • PolymyalgiaRheumatica. Saad, Fioravanti, Samuels. Emedicine. Updated Aug 20, 2009 • Arch Intern Med. 2009 Nov 9;169(20):1839-50. Treatment of PMR: a systematic review. Hernandez-Rodriguez. • Lancet. 2008 Jul 19;372(9634):234-45. PMR and Temporal Arteritis. Salvarani et al.