Download
1 / 107
1.08k likes | 1.32k Vues
Physiological Approach of Arrythmia. M. Saifur Rohman , dr SpJP , PhD. FICA. OUTLINE. Membrane potential, action potential, impulse conduction, type of arrhytmias, cause of arrhytmias,. Electrical Activity of Heart.

E N D
Physiological Approach of Arrythmia M. SaifurRohman, drSpJP, PhD. FICA
OUTLINE • Membrane potential, • action potential, • impulse conduction, • type of arrhytmias, • cause of arrhytmias,
Electrical Activity of Heart • Heart beats rhythmically as result of action potentials it generates by itself (autorhythmicity) • Two specialized types of cardiac muscle cells • Contractile cells • 99% of cardiac muscle cells • Do mechanical work of pumping • Normally do not initiate own action potentials • Autorhythmic cells • Do not contract • Specialized for initiating and conducting action potentials responsible for contraction of working cells
Elektrokardiogram (EKG) • Rekaman grafik potensial listrik yang dihasilkan oleh jaringan jantung Goldman & Goldschlager Cara Perekaman EKG : • Permukaan • Epikardial • Endokardial / intrakardial
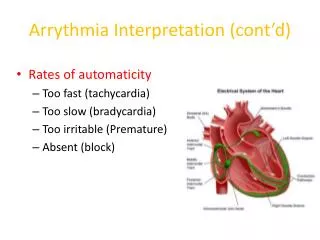
Electro-Physiology of the Heart • Electrophysiologic properties (regulates heart rate & rhythm) - Automaticity – ability of all cardiac cells to initiate an impulse spontaneously & repetitively - Excitability – ability of cardiac cells to respond to stimulus by initiating an impulse (depolarization) - Conductivity – cardiac cells transmit the electrical impulses they receive - Contractility – cardiac cells contract in response to an impulse - Refractoriness – cardiac cells are unable to respond to a stimulus until they’ve recovered (repolarized)
Intrinsic Cardiac Conduction System Approximately 1% of cardiac muscle cells are autorhythmic rather than contractile 70-80/min 40-60/min 20-40/min
Sinoatrial (SA) Node • Normal cardiac impulse originates here • “Natural pacemaker” • Inherent rate: 60-100 bpm • Atrial depolarization occurs cell to cell • Four conduction pathways transmit impulse to AV node: Bachman’s Bundle and 3 internodal pathways (anterior, middle & posterior tracts). • Spreads impulse throughout the atrium
Atriovenous (AV) Node • Located inferiorly in RA • All impulses initiated in atria will be conducted to ventricles via AV node alone. • Impulse slows here to allow diastolic filling time • Inherent rate: 40-60 bpm • Conduction delay at AV node so that ventricular filling from atrial contraction
Bundle of HIS • Electrical impulses conducted to ventricles via Bundle of HIS & purkinjie fibers • Divides into bundle branches • Right • Left • Anterior Fascicle • Posterior Fascicle
Purkinje Fibers • Impulse stimulates ventricular myocardial cells • Inherent rate: 20-40 bpm
Intrinsic Conduction System • Autorhythmic cells: • Initiate action potentials • Have “drifting” resting potentials called pacemaker potentials • Pacemaker potential - membrane slowly depolarizes “drifts” to threshold, initiates action potential, membrane repolarizes to -60 mV. • Use calcium influx (rather than sodium) for rising phase of the action potential
Pacemaker Potential • Decreased efflux of K+, membrane permeability decreases between APs, they slowly close at negative potentials • Constant influx of Na+, no voltage-gated Na + channels • Gradual depolarization because K+ builds up and Na+ flows inward • As depolarization proceeds Ca++ channels (Ca2+ T) open influx of Ca++ further depolarizes to threshold (-40mV) • At threshold sharp depolarization due to activation of Ca2+ L channels allow large influx of Ca++ • Falling phase at about +20 mV the Ca-L channels close, voltage-gated K channels open, repolarization due to normal K+ efflux • At -60mV K+ channels close
PX = Permeability to ion X PNa 1 +20 2 PK and PCa 0 -20 PK and PCa 3 0 -40 Membrane potential (mV) PNa -60 -80 4 4 -100 0 100 200 300 Time (msec) Phase Membrane channels 0 Na+ channels open 1 Na+ channels close 2 Ca2+ channels open; fast K+ channels close 3 Ca2+ channels close; slow K+ channels open 4 Resting potential AP of Contractile Cardiac cells • Rapid depolarization • Rapid, partial early repolarization, prolonged period of slow repolarization which is plateau phase • Rapid final repolarization phase
AP of Contractile Cardiac cells • Action potentials of cardiac contractile cells exhibit prolonged positive phase (plateau) accompanied by prolonged period of contraction • Ensures adequate ejection time • Plateau primarily due to activation of slow L-type Ca2+ channels
Why A Longer AP In Cardiac Contractile Fibers? • We don’t want Summation and tetanus in our myocardium. • Because long refractory period occurs in conjunction with prolonged plateau phase, summation and tetanus of cardiac muscle is impossible • Ensures alternate periods of contraction and relaxation which are essential for pumping blood
Ion movement and channels • The movement of specific ions across the cell membrane serve as action potentials depends on : • 1. Energetic favorability; concentration gradient and transmembrane potential • 2. Permeability of the membrane for the ion: channels which is selective and gated • Selective: manifestation of size and structure of its pore • Gated: pass through it specific channels only at certain times; voltage sensitive gating (fast sodium channel)
Electrical to mechanical response • Excitation-contraction coupling • During phase 2 of the action potential Ca enter through L Type Ca Channel in the sarcolemma and T tubule • Ca triggers release much greater Ca from SR via Ryanodine receptor into cytosol result in an increased Ca in the cytosol • Ca bind to Trop C and the activity of Trop I is inhibited and induce conformational change of tropomyosin result in unblock the active site between actin and myosin • Myosin head bind to actin causing interdigitating thick and thin filament in ATP dependent reaction
Electrical Signal Flow - Conduction Pathway • Cardiac impulse originates at SA node • Action potential spreads throughout right and left atria • Impulse passes from atria into ventricles through AV node (only point of electrical contact between chambers) • Action potential briefly delayed at AV node (ensures atrial contraction precedes ventricular contraction to allow complete ventricular filling) • Impulse travels rapidly down interventricular septum by means of bundle of His • Impulse rapidly disperses throughout myocardium by means of Purkinje fibers • Rest of ventricular cells activated by cell-to-cell spread of impulse through gap junctions
1 1 SA node AV node 2 1 THE CONDUCTING SYSTEM OF THE HEART SA node depolarizes. 2 Electrical activity goes rapidly to AV node via internodal pathways. SA node 3 Internodal pathways 3 Depolarization spreads more slowly across atria. Conduction slows through AV node. AV node 4 Depolarization moves rapidly through ventricular conducting system to the apex of the heart. A-V bundle 4 Bundle branches Purkinje fibers Depolarization wave spreads upward from the apex. 5 5 Purple shading in steps 2–5 represents depolarization. Electrical Conduction in Heart • Atria contract as single unit followed after brief delay by a synchronized ventricular contraction
Excitation-Contraction Coupling in Cardiac Contractile Cells • Ca2+ entry through L-type channels in T tubules triggers larger release of Ca2+ from sarcoplasmic reticulum • Ca2+ induced Ca2+ release leads to cross-bridge cycling and contraction
P wave: atrial depolarization START P The end R PQ or PR segment: conduction through AV node and A-V bundle T P P QS Atria contract. T wave: ventricular Repolarization ELECTRICAL EVENTS OF THE CARDIAC CYCLE Repolarization R T P QS Q wave P Q ST segment R R wave P R Q S P R Ventricles contract. Q P S wave QS Heart Excitation Related to ECG
Electrocardiogram (ECG) • Record of overall spread of electrical activity through heart • Represents • Recording part of electrical activity induced in body fluids by cardiac impulse that reaches body surface • Not direct recording of actual electrical activity of heart • Recording of overall spread of activity throughout heart during depolarization and repolarization • Not a recording of a single action potential in a single cell at a single point in time • Comparisons in voltage detected by electrodes at two different points on body surface, not the actual potential • Does not record potential at all when ventricular muscle is either completely depolarized or completely repolarized
Electrocardiogram (ECG) • Different parts of ECG record can be correlated to specific cardiac events
Batasan dan Pembagian Aritmia Pada umumnya aritmia dibagi menjadi 2 golongan besar : • Gangguan pembentukan impuls • Gangguan penghantaran impuls
Irama Sinus Normal • Gelombang P : - harus ada - mendahului kompleks QRS - positif di II, aVF - inverted di aVR • Interval PR : - durasi 0,12- 0,20 detik dan konstan • Kompleks QRS : - durasi < 0,10 detik • Frekuensi 60-100/menit
Gangguan Pembentukan Impuls a.Gangguan pembentukan impuls di sinus 1. Takikardia sinus 2. Bradikardia sinus 3. Aritmia sinus 4. Henti sinus
Takikardia Sinus Kriteria : irama sinus, rate > 100/menit
Bradikardia Sinus Kriteria : irama sinus, rate < 60/menit
Aritmia Sinus Pengaruh respirasi melalui stimulasi reseptor saraf vagus di paru Akhir inspirasi : frekuensi > cepat, akhir ekspirasi frekuensi > lambat
Aritmia Sinus Perbedaan rate maksimum dan minimum > 10 % atau > 120 mdet Rate maks- rate min/ rate min > 10 %
HentiSinus Tak ada gelombang P dari sinus
Gangguan Pembentukan Impuls b. Pembentukan impuls di atria (aritmia atrial) 1. Ekstrasistol atrial 2. Takikardia atrial 3. Gelepar atrial 4. Fibrilasi atrial
Ekstrasistol Atrial Kriteria : - gelombang P prematur dari atrium - biasanya pause kompensasi tak lengkap
Tipe EkstrasistolAtrial Couplet : 2 EA, Takikardia atrial : 3 atau lebih EA Bigemini : 1 kompleks sinus diikuti 1 EA Trigemini : 2 kompleks sinus diikuti 1 EA
Atrial ekstrasistol unifokal, multifokal dan wandering atrial pacemaker Unifokal : satu fokus ektopik Multifokal : 2 atau lebih fokus ektopik Wandering PM : fokus ektopik berbeda-beda