Download
1 / 29
310 likes | 596 Vues
D- Selection of Antihypertensive Drug. Selection of Antihypertensive Drug. Alpha Blocker. AT 1 Antagonist. α 2 - agonists. ACE Inhibitor. Ganglionic blockers. Dr. Rx Rational. Drug of choice. Beta Blocker. Vasodilators. Ca ++ Antagonist. Diuretic. 1. 2. 3.

E N D
Selection of Antihypertensive Drug Alpha Blocker AT1Antagonist α2- agonists ACE Inhibitor Ganglionicblockers Dr. Rx Rational Drug of choice BetaBlocker Vasodilators Ca++ Antagonist Diuretic
1 2 3 Selection of Antihypertensive Drug Level of blood pressure + Presence of other risk factors for CVD & target organ damage + Coexisting diseases Antihypertensive Therapy
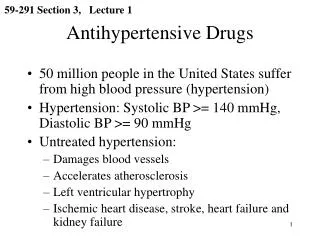
Pharmacotherapy of Hypertension • Target organ damage/clinical CVD • LVH- Heart failure- Angina- Prior MI or revasculaization • Stroke or TIA, • Retinopathy, • Peripheral Vascular Disease • Nephropathy,
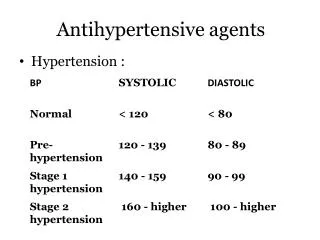
SBP DBP mm Hg mmHg JNC 7 Blood Pressure Classification • Normal • Prehypertensive • Stage 1 Hypertension • Stage 2 Hypertension <120 and <80 120-139 or 80-89 140-159 or 90-99 > 160 or > 100
SBP DBP mm Hg mmHg JNC 7 Goal Blood Pressure • Most patients • Diabetes • Chronic Renal Disease < 140 < 90 < 130 < 80 < 130 < 80
JNC 7 Approximate SBP Reduction mmHg Lifestyle Modifications • Weight reduction • DASH eating plan • Reduced Sodium Intake • Physical activity • Moderation of alcohol consumption 5 – 20 8 – 14 2 – 8 4 – 9 2 – 4
Not at Goal Blood Pressure JNC 7 Lifestyle Modifications Initial Drug Choices Algorithm for Treatment of Hypertension
JNC 7 Initial Drug Choices “Excellent clinical trial outcome data prove that lowering BP with several classes of drug, including ACE inhibitors, angiotensin receptors blockers (ARBs),”beta-blockers”, calcium channel blockers (CCBs) and thiazide-type diuretics will reduce the complications of hypertension.” Algorithm for Treatment of Hypertension
JNC 7 Initial Drug Choices Without Compelling Indication (s) With Compelling Indication (s) Algorithm for Treatment of Hypertension
Stage 1- Hypertension 140-159 / 90-99 mmHg Without Compelling Indication Thiazide-like diuretics for most, ACEI, ARB, BB or CCB May consider combination JNC 7 Initial Drug Choices Algorithm for Treatment of Hypertension
Stage 2 - Hypertension >160 / >100 mmHg Without Compelling Indication 2-drug combination for most Usually thiazide-like diuretic plus ACEI, or ARB, or BB or CCB JNC 7 Initial Drug Choices Algorithm for Treatment of Hypertension
Without Compelling Indication (s) With Compelling Indication (s) Not at Goal Blood Pressure Initial Drug Choices Optimize dosage or add additional drug until goal BP is achieved. Consider consultation with HNT specialist JNC 7 Algorithm for Treatment of Hypertension
Clinical trial and guideline basis for compelling indications for individual drug classes
Hypertension in Elderly • Pharmacological treatment: - Lower initial doses (1/2 dose than in younger patients) - The reduction in BP should be gradual - Greater caution in patients with co-existing diseases or orthostatic hypotension. • Choice of therapy: - Thiazide diuretic (hydrochlorothiazide, HCTZ 12.5 mg) - STOP-Hypertension trial: ACE inhibitors, long-acting calcium antagonist and beta- blockers may provide the same protection as diuretics.
Hypertension in Elderly • Choice of therapy: special considerations • A diuretic should be used for heart failure or edema • A beta-blocker should be used for patient with coronary heart disease, tachyarrhitmias or migraine • An ACE inhibitors in patients with heart failure • Calcium antagonist should be used in patients with angina pectoris,and peripheral vascular disease • Alpha-blocker in patient with benign prostatic hyperplasia
Hypertension and Diabetes • Treatment: • Early treatmentto prevent cardiovascular disease • and minimize progression of renal and retinal disease. • The benefits oftight blood pressure controlin diabetics may be as great or greater than benefits of strict glycemic control. • Initial therapy should includenon-pharmacological methods. • ACE Inhibitors, ARBs, C++ Channel Blockers,
Hypertension and Diabetes • Kidneys in diabetic patients are more sensitive • to any increase in blood pressure • Proteinuria is not only the marker of renal damage, • but also risk factor for progression of renal disease Pathogenesis:
Asthma COPD and Hypertension • Beta-blockers (i) increase bronchial obstruction, • (ii) increase in airways reactivity, and (iii) inhibit the bronchodilatatory effects of beta agonist • Cardioselective, beta-blockers none should be considered safe.Even topical administration for the treatment of glaucoma may led to asthmatic exacerbations. • ACE inhibitors are not contraindicated and may be used; very rarely worsen airflow obstruction; produce persistent dry cough and are not first line drug for hypertensive patients with asthma or COPD.
Asthma COPD and Hypertension • Diuretics: can be effectively used but there is an increased risk of hypokalemia (inhaled β-2 agonist drive potassium into cell and orally administered corticosteroids mildly increase urinary potassium excretion). • Only low dose (12.5-25 mg) of thiaizides to be used. • In patients with COPD and chronic hypercapnia, diuretics-induced metabolic alkalosis may suppress the ventilatory drive and exacerbates the hypoxia.
Asthma, COPD and Hypertension Calcium channel blockers (CCB) are preferred for treatment of hypertension in astma & COPD. May be combined with diuretics Short-acting CCB (niphedipine) should not be used because they increase CV risk. Only long-acting CCB or slow-release niphedipine formulation should be used.
Ischemic Heart Disease and Hypertension • IHD is the most common form of target-organ damage associated with hypertension. • Beta blockers and long acting Ca++ channel blockers are the first choice in HTN patient with stable angina pectoris. • HTN patients with unstable angina or MI should be treated with beta blocker or ACE inhibitor. • In patients with post-myocardial infarction, ACE inhibitors, beta blockers and aldosterone antagonists; all reduce progression of left ventricular dysfunction and mortality.
Hart Failure and Hypertension • ACE inhibitors and beta blockers are recommended for HTN patients with asymptomatic ventricular dysfunction • In HTN patients with symptomatic ventricular dysfunction (NYHA III and IV) in addition to ACE inhibitors and beta blockers, treatment with diuretics, Ang II receptor antagonists and aldosterone antagonists. • In hypertensive HF patient, if volume depleted, ACE inhibitors may induce hypotension and acute renal failure. Beta blockers may induce initial/transient worsening of HF.
Pharmacotherapy of Hypertension • Pregnancy : Methyl Dopa, Hydralazine • Gout & Dyslipidemia: Avoid diuretics • Benign prostatic hypertrophy: Alfa-1 adrenergic • blockers
Pharmacotherapy of Hypertension Alpha Blocker AT1Antagonist α2- agonists ACE Inhibitor Ganglionicblockers Drug of choice BetaBlocker Vasodilators Ca++ Antagonist Diuretic