Overview of Glaucoma
670 likes | 965 Vues
Overview of Glaucoma. Michael J. Siegel, M.D. Kresge Eye Institute Detroit Medical Center/Wayne State University. Glaucoma Defined: Characteristic Optic Neuropathy with physiologic (visual field) or anatomic (nerve fiber layer) deviations from normal.

Overview of Glaucoma
E N D
Presentation Transcript
Overview of Glaucoma Michael J. Siegel, M.D. Kresge Eye Institute Detroit Medical Center/Wayne State University
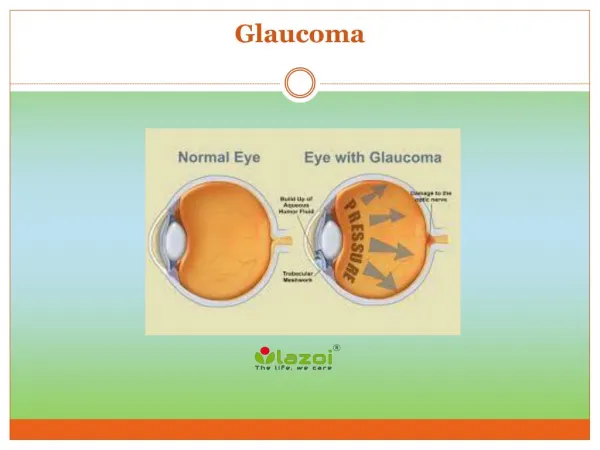
Glaucoma Defined: Characteristic Optic Neuropathy with physiologic (visual field) or anatomic (nerve fiber layer) deviations from normal.
Basic Glaucoma Classification(Based on Outflow Mechanism) • Primary (Chronic) Open Angle • Closed/Narrow Angle • Primary • Pupillary Block • Non-Pupillary Block (Plateau Iris) • Secondary • Developmental • Glaucoma from Systemic Disease
. American Academy of Ophthalmology Basic and Clinical Science Course: Glaucoma: Section 10: AAO, San Francisco, 2010.
Allingham R, et al. Shields Textbook of Glaucoma; LW&W, New York. 2010.
Developmental Glaucoma These glaucoma's are not readily separated into open-angle and angle-closure mechanisms, but typically represent incomplete development of structures in the conventional aqueous outflow pathway. High insertion of the anterior uvea, as in congenital (infantile) glaucoma Incompletely developed TM or Schlemm (e.g., Peters anomaly) Iridocorneal adhesions (e.g., Axenfeld-Rieger syndrome).
Chronic Open Angle Glaucoma's in which the anterior chamber angle structures (i.e., trabecular meshwork, scleral spur, and ciliary body band) are visible by gonioscopy. • Anterior Chamber Mechanisms • Pre-trabecular • Trabecular • Distal to Meshwork (Schlemm’s Canal) • Post-Trabecular
POAG Characteristics Bilateral but not always symmetric Characteristic Optic Nerve and Visual Field damage Adult Onset Open and normal appearing anterior chamber angles on gonioscopy Absence of secondary causes
POAG: Groups at Risk • Elderly • African-Americans • Positive Family History of POAG • Individuals with: • Elevated IOP on exam (Ocular Hypertension) • High Myopia (Nearsighted) • Thin Pachymetry (Thin Cornea) • CAD/CVD/HTN/DM - ? association
POAG and African Americans • Blindness is 3x-4x more common • Age >70 equals 10% prevalence vs. 2% for Caucasians • POAG tends to occur at earlier age • POAG tends to be more advanced when discovered
POAG Risk Factor: Elevated IOP • Elevated IOP correlates directly with optic nerve damage • Corneal Thickness • Thin – Higher Risk; measured IOP is lower than actual • Thick – Lower Risk; measured IOP is higher than actual
Pre-Trabecular Trabecular Post-Trabecular Allingham R, et al. Shields Textbook of Glaucoma; LW&W, New York. 2010.
Glaucoma Suspects Normal Visual Fields Open and Normal Appearing Angles + Elevated IOP and/or Enlarged Cup to Disc Ratio
Glaucoma: Optic Nerve Changes Increased cup to disc ratio Thinning of disc rim Progressive loss of neural rim tissue Loss of nerve fibers Disc Hemorrhages
Beta Blockers • Relative B1 selective vs. nonselective –BID dosing • May use qd in controlled patients • Decrease aqueous production • Serum half life differs from ocular duration-wash out of 2 weeks • Systemic side effects and cross over effects • Short term escape and long term drift.
Adrenergic Agonist • Non-selective – epinephrine, and dipivefrin – pro-drug of epinephrine. • Selective alpha 2- clonidine, apraclonidine (iopidine), and brimonidine (alphagan). • Alpha 2 mediated decrease in blood flow to the cilliary body and decreased aqueous production. • Nonselctive side fx: numerous surface problems including conjunctivitis and adrenochrome deposits
Selective Adrenergic Agonist • Alpha 2 agonist have less systemic and local side effects. • Clonidine causes systemic side fx that make it poorly suited for the treatment of glaucoma. • Apraclonidine- good for post operative pressure management but high rate of allergy and loss of efficacy. • Bromonidine- less local side fx but still present including conjunctivits – generic 0.2%.
Cholinergic Agents • Lower IOP by increasing aqueous outflow • Ach in the eye contracts the longitudinal muscle of CB – also the circular muscle and iris sphincter producing accommodation • Muscle contraction widens trabecular spaces • Side fx limit use- induced myopia, accommodative spasm (headache), RD, cataract, aggravation of ocular inflammation.
Cholinergic Agents • Indirect agents act on cholinesterase – Ecothiophate (phospholine iodide), physostigmine (eserine), demecarium (humersol) • Indirect agent also block pseudocholinesterase which metabolizes succinylcholine – these agents must be stopped 2 weeks prior to OR. • Direct agents Pilocarpine, carbachol (miostat), acetylcholine (miochol).
Oral Carbonic Anhydrase Inhibitors • Acetazolamide (diamox) 125,250,500mg • Methazolamide (neptazane) 25, 50mg – possibly safer in renal dx. With less systemic side effects.
Oral Carbonic Anhydrase Inhibitors • Nine isoenzymes of the CA and CA-II predominates in the ciliary processes. • Systemic side effect limit use in elderly with 50% unable to tolerate. • Acidosis, K+ depletion, GI upset, metalic taste, weight loss, urolithiasis, parasthesias, headache, malaise, anemia, stevens-johnson • Do not use in renal failure, respiratory acidosis, sickle cell, pregnancy and lactation.
Topical Carbonic Anhydrase Inh. • Dorzolamide (Trusopt) – also in combination with timolol (Cosopt) BID or TID dosing may limit use in eyes with endothelial issues. • Brinzolamide (Azopt) –Less surface irritation.
Prostaglandin Analogs • Latanoprost (xalatan), travaprost (travatan), bimataprost (lumigan) • Increase Uvealscleral outflow • Good for combination therapy • Ocular side fx:hyperemia, iris pigmentation (caution in heterochromic iris) • CME and iritis cases
Glaucoma: Surgical Procedures • Laser Surgery (ALT/SLT) • Filtering Surgery (Trabeculectomy, EX-Press) • Drainage Device (Molteno, Ahmed, BaerveldtValves • Cyclodestructive Procedures (ECP, Trans-scleral) • Angle Destructive Procedures (Trebeculotomy, Goniotomy)
. American Academy of Ophthalmology Basic and Clinical Science Course: Glaucoma: Section 10: AAO, San Francisco, 2010.
Angle Closure GlaucomaThe Confusion… Membrane Pulling the Iris into the Angle Pulled Iris or Anterior Mechanism Pushed Iris or Posterior Mechanism Allingham R, et al. Shields Textbook of Glaucoma; LW&W, New York. 2010.
Angle Closure Glaucoma: High Risk Groups Elderly Eskimos/Inuit Asians Females Hyperopic Patients (Farsighted Patients) Positive Family History of Angle Closure