Download
1 / 23
230 likes | 494 Vues
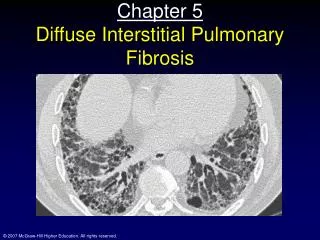
Chapter 5 Diffuse Interstitial Pulmonary Fibrosis. Topics. Pathology of diffuse interstitial pulmonary fibrosis Normal alveolar wall structure Reduced lung volumes and compliance Pressure-volume curves Diffusion across the blood-gas barrier Diffusing capacity. Case Study #5: Elena.

E N D
Topics • Pathology of diffuse interstitial pulmonary fibrosis • Normal alveolar wall structure • Reduced lung volumes and compliance • Pressure-volume curves • Diffusion across the blood-gas barrier • Diffusing capacity
Case Study #5: Elena • 40 yr old Blues singer • Dyspnea and fatigue • 5 years ago symptoms worsened • Weight loss and unusual fatigue • Irritating, unproductive cough • No family history of pulm disease • No apparent toxic exposure
Physical exam #5: Elena • Drawn • Rapid, shallow breathing • Poor inspiratory movement • Crackles on inspiration • Clubbed fingers • Loud pulmonary second sound (indicative of R side HF)
Investigations • Normal hemoglobin and cell counts • Small contracted lung and rib cage • Raised diaphragm
Exercise and pulm function tests • Vo2 max: 2.2 L/min • Stopped because of SOB • Look at very low Po2 values • Why? • DLCO
Lung Biopsy • Definitive diagnosis • Marked thickening of alveolar walls • Extensive collagen deposition • Capillary obliteration • Cause: unknown
Normal histology and Pathology • Restrictive lung disease • No obstruction • Small volumes • Interstitial disease affects the parenchyma (tissue) • Normal vs. restrictive alveolar wall
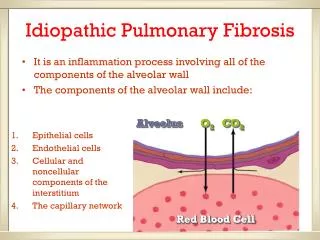
Alveolar anatomy • Normally • Blood-gas barrier: ~ 0.3 um • Alveolar epithelium, interstitium, capillary endothelium • Type I cell • Chief structural cell of alveoli • Structural • Collagen • Type II cell • Epithelial • Globular • Little structural support • Metabolically active • Forms surfactant • In injury, transformed into type I cells
Alveolar anatomy II • Other cells • Macrophages • Scavenge foreign particles and bacteria • Fibroblasts • Synthesize collagen and elastin • In fibrosis; large amts of collagen are laid down in interstitium of alveolar wall
Alveolar anatomy III • Interstitium • Space between alveolar epithelium and capillary endothelium • Usu. Thin • Provides integrity and strength to BG barrier • Vulnerable to stress
Pathology of Diffuse Interstitial Pulmonary Fibrosis • Many synonyms • Idiopathic pulmonary fibrosis • Interstitial pneumonia (inflammation and flooding) • Cryptogenic fibrosing alveolitis • Principal features • Thickening of the interstitium • Collagen deposition • Infiltration with lymphocytes • Fibroblasts lay down collagen • Desquamation: cellular exudate (containing macrophages) in alveoli • Destruction of alveolar architecture • “Honeycomb” lung; scarring of lung (resists stretching)
Physiology and pathophysiology • Clinical findings • Chief complaint: dyspnea • Caused by stiff lung • Reduced compliance • Shallow, rapid breathing • Physical exam • Crepitations on inspiration caused by fibrotic lesions • Loud 2cd pulmonary sound: hypertension • Caused by wholesale destruction of pulm caps • Chest radiograph • Small lung
Pulmonary function tests • Right shifted compliance curve (low) • Very low lung volumes
Pulmonary function in fibrosis • Relaxation pressure-volume curve • Fig 5-6 • FRC: lung and chest wall forces are equal • Above FRC: • Lung+chest wall forces are positive • Greater tendency for recoil • Below FRC: • They are negative • Greater tendency for expansion • Obstructive disease: FRC increases; why? • Restrictive disease: FRC decreases; why?
Forced expiration • FVC decreased • FEV1.0/FVC: normal • Elevated FEF25-75% • Rapid exhalation; why? • Little dynamic compression • Scarring supports the airways and holds them open
Arterial blood gases • Hypoxemia; why? • VA/Q mismatch • Destruction of capillaries • Derangement of alveolar architecture • Diffusion limitation • Thickened BG barrier
Diffusion across Blood-gas barrier • Diffusion limitation vs perfusion limitation • CO: diffusion limited • Binds very strongly to Hb • Thus, partial pressure changes very little; why? • No back-pressure • Transfer limited by properties of blood-gas barrier • N2O: perfusion limited • NO combination with Hb • Dissolves in plasma • Partial pressure rises rapidly • Transfer limited by blood flow • O2? • Can be both
Diffusion across Blood-gas barrier • So, O2 is perfusion limited in health, where the rise in partial pressure is rapid due to the lower affinity of Hb for O2 and the very high diffusing capacity • In disease, when the diffusion capacity is reduced, then O2 becomes diffusion limited • Also, diffusion of a gas depends upon it’s solubility in both the BG barrier AND the blood • If the same, no diffusion limitation • If different, diffusion limited • Thus, BG barrier thickness increase can limit diffusion
Measurement of diffusing capacity • Carbon monoxide: • Diffusion limited gas • V gas = A/T x (P1-P2) x D • V gas = DL (P1-P2) • DL = diffusing capacity of the lung • Includes area, thickness and diffusive properties of membrane and gas • DL = Vco/(P1-P2) • DL = Vco/PAco • Vol of CO transferred per unit pressure CO
Measurement of diffusing capacity • Usu. Subject takes a breath of dilute CO mixture (0.3%) and exhales • Conc difference between inspired and exhaled measured; rate of disappearance measured • Rx rate with Hb • Not all resistance to transfer lies in membrane • Some lies in the Rx rate with Hb • Two stages • Diffusion through BG barrier (includes plasma and RBC membrane) • Rx rate with Hb
Measurement of diffusing capacity • These two “resistances” produce the overall “resistance to diffusion” • Overall “conductance” is the inverse of these resistances (see Fig. 5-9) • DL = diffusing capacity of the lung • DM = diffusing capacity of the “membrane” • Θ = rx rate with Hb • Vc = capillary blood vol
Why is Elena’s diffusing capacity reduced? • Reduced membrane conductance • Reduced Vc • Perhaps also due to unequal VA/Q