SINDROME DE CUSHING (HIPERCORTISOLISMO)
970 likes | 4.18k Vues
SINDROME DE CUSHING (HIPERCORTISOLISMO). PROFESOR TITULAR DR DIAZ GREENE PROFESOR ADJUNTO DR RODRIGUEZ WEBER SUPERVISÓ: R1MI GRETA REYES MÓDULO ENDOCRINOLOGIA 20 ABRIL 2010. Harvey W. Cushing (1869-1939). Science Museum's History of Medicine website. MINERALOCORTICOIDES: ALDOSTERONA.

SINDROME DE CUSHING (HIPERCORTISOLISMO)
E N D
Presentation Transcript
SINDROME DE CUSHING(HIPERCORTISOLISMO) PROFESOR TITULAR DR DIAZ GREENE PROFESOR ADJUNTO DR RODRIGUEZ WEBER SUPERVISÓ: R1MI GRETA REYES MÓDULO ENDOCRINOLOGIA 20 ABRIL 2010
Harvey W. Cushing(1869-1939) Science Museum's History of Medicine website
MINERALOCORTICOIDES: ALDOSTERONA GLOMERULAR GLUCOCORTICOIDES: CORTISOL CORTEZA FASCICULADA ANDRÓGENOS RETICULADA MÉDULA CATECOLAMINAS
ETIOLOGÍA Aumento en la producción cortisol por la suprarrenal. Causa mayoría: hiperplasia suprarrenal bilateral (ACTH: hipófisis, ectópica, tumor). ♀ 3x 3ª a 4ª década 90% dependiente tumor hipofisiario Defecto primario: desarrollo de novo de adenoma Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
ETIOLOGÍA Enfermedad de Cushing: tumor hipofisiario productor de ACTH Síndrome de Cushing: todas las causas de exceso de cortisol: • Tumor ACTH exógeno • Tumor suprarrenal • Tumor hipofisiario secretor ACTH • Tratamiento con exceso de glucocorticoides Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
ETIOLOGÍA 1. TUMOR ACTH ECTÓPICO: • Tumores no hipofisiarios • Hiperplasia suprarrenal bilateral • Signos y síntomas presentes o no. • Alcalosis hipopotasémica Carcinoma broncógeno cel. pequeñas, carcinoides: timo, páncreas, ovario, medular tiroideo; adenomas bronquiales. Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
ETIOLOGÍA 2. TUMOR SUPRARRENAL • 20-25% en Sx Cushing • Unilaterales • 50% malignos Puede: hipersecreción hipofisiaria → hiperplasia nodular suprarrenales Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
ETIOLOGÍA 3. TUMOR HIPOFISIARIO SECRETOR ACTH Micro o macroadenomas 50% , 5 mm 4. YATROGENIA Causa más frecuente Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
Evaluation of health-related quality of life in patients with Cushing's syndrome with a new questionnaire". Webb, SM; Badia, X; Barahona, MJ; Colao, A; S trasburge, CJ; Tabarin, A; van Aken, MO; Pivonello, R; Stalla, G; Lamberts, SWJ; Glusman, JE. EUROPEAN JOURNAL OF ENDOCRINOLOGY, 158 (5): 623-630 MAY 2008.
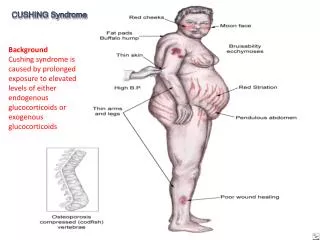
SIGNOS Y SÍNTOMAS • Glucocorticoides: catabolismo • Debilidad muscular • Fatiga • Osteoporisis • Estrias • Equimosis • Gluconeogénesis, resistencia insulina • Deposito tejido adiposo: cara, interescapular, lecho mesentérico • Hipertensión • Cambios emocionales, depresión , psicosis • Acné , hirsutismo, oligomenorrea
Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO Fundamento: Demostrar ↑ cortisol, × suprimirlo con dexametasona. No hay prueba que supere 95% especificidad. Pruebas iniciales: • SUPRESIÓN NOCTURNA: 1gr. dexa a las 00:00 hrs Cortisol 8:00 hrs >5 μg/100ml Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO 2. OBESOS O DEPRIMIDOS Cortisol urinario en 24 horas >50 μg/día---sospecha 3. Definitivo: Dexa .5mg c/6hr por 48 hrs cortisolurin no baja de 10μg, o si cortisolplasm no baja de 5 μg/100ml Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO …tomando en cuenta a ACTH, sirve para distinguir las diversas causas ( dependiente o independiente de ACTH). Tumores suprarrenales: niveles ACTH bajos o indetectables ( menos 10pg/ml) ACTH ectópica: mas 500 pg/ml Microadenoma o disfunción H-H, ACTH 30-150 pg/ml (normal <60 pg/ml) Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO Distinción de microadenoma secretor ACTH vs. Disfunción H-H, otras: Reacción cortisol ante dexa 2mg c/6h por 48 hrs o 8 mg dexa durante la noche Prueba supresión con dosis elevadas: Especificidad cercana 100%, si la supresión en mas 90% de cortisol libre en orina. Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO Otras pruebas: Metirapona y Goteo CRH “si hay hipersecreción de esteroides por tumor suprarrenal, o producción ectópica de ACTH, debe causar supresión del eje H-H Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO El dilema del diagnostico principal: Consiste en distinguir entre los casos por microadenomas de hipófisis, fuentes ectópicas a los que producen CRH, ACTH o ambas. Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO Si estudios de imagen son negativos: Determinación de ACTH en sangre de seno petroso, midiendo concentración basal, a los 2.5 y 10 minutos después de administrar CRH (1μg/kg IV): Si periférica mayor de 3, confirma tumor hipofisiario. Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO Adenoma suprarrenal productor de cortisol: ACTH baja Cortisol libre en orina ↑ ↑ ↑ Carcinoma suprarrenal Masa abdominal palpable 17-cetoesteroides urinarios ↑ ↑ ↑ Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO DIFERENCIAL SINDROME SEUDO CUSHING Obesidad, alcoholismo, depresión. Elevación moderada de cortisol en orina Resistencia prueba supresión Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO DIFERENCIAL Sindrome Cushing leve versus Seudo-Cushing Dexa dosis bajas en 2 dias, alta sensibilidad y especificidad. Yatrógeno, megestrol: clínicamente indistinguible de hiperfunción suprarrenal. Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
DIAGNÓSTICO DIFERENCIAL Prueba de cortisol en saliva ( nocturna) The Journal of Clinical Endocrinology & Metabolism 91(10):3746–3753 CLINICAL REVIEW: Cushing’sSyndrome: ImportantIssues in Diagnosis and Management
DIAGNÓSTICO DIFERENCIAL La intensidad de SxCushingyatrógeno depende de : • Dosis total • Vida media biológica • Duración tratamiento Mañana y tarde: ↑↑↑ Mañana: ↑↑ Tomografía, mejor técnica (Tumores e hiperplasia) Hipersecresiónhipofisiaria: RMN Producción ectópica ACTH: Tomografía tórax. Harrison's Online > Chapter 336. Disorders of the Adrenal Cortex >
TRATAMIENTO Neoplasia suprarrenal: Extirpación tumor Previa preparación ( insuficiencia ): Diario: 20mg-10mg-0.1 1 día antes cx: 20-10-0.1 Día cirugía: 10 mg/hra Dia 1-7: 5-7.5,2.5-5,2.5-5 + 40-20-0.1,2.5-5 + 40-20-0.1, 40-20-0.1, 20-20-0.1, 20-10-0.1.
TRATAMIENTO Carcinoma suprarrenal: mueren 3 años después de diagnóstico, metástasis hígado y pulmón. Mitotano ( isómero DDT [DicloroDifenilTricloroetano]): inhibe formación cortisol. • 3 a 4 tomas al día, aumentando a tolerancia (6g/día) . • 1/3 retroceso tumor primario • Metástasis no son sensibles Platino.