Download
1 / 37
480 likes | 1.15k Vues
Prevalence of Anxiety Disorders. Kessler et al. Arch Gen Psychiatry . 1995;52:1048. Kessler et al. Arch Gen Psychiatry . 1994;51:8. Outcome of Panic Disorder at Long-Term Follow-up. Roy-Byrne & Cowley, 1995. Pharmacopoeia for Anxiety Disorders. Antidepressants

E N D
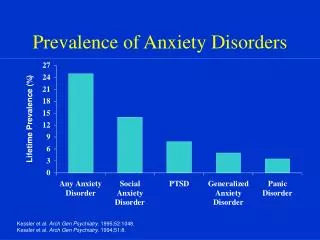
Prevalence of Anxiety Disorders Kessler et al. Arch Gen Psychiatry. 1995;52:1048. Kessler et al. Arch Gen Psychiatry. 1994;51:8.
Outcome of Panic Disorder at Long-Term Follow-up Roy-Byrne & Cowley, 1995
Pharmacopoeia for Anxiety Disorders Antidepressants Serotonin Selective Reuptake Inhibitors (SSRIs) Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) Atypical Antidepressants Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Benzodiazepines Other Agents Azaspirones Beta blockers Anticonvulsants Other strategies
Serotonin Selective Reuptake Inhibitors • Fluoxetine (Prozac), 20-80 mg/d • Initiate with 5-10 mg/d • Sertraline (Zoloft), 50-200 mg/d • Initiate with 25-50 mg/d • Paroxetine (Paxil), 20-50 mg/d • Initiate with 10mg/d • Fluvoxamine (Luvox), 50-300 mg/d • Initiate with 25 mg/d • Citalopram (Celexa) - Initiate with 10-20 mg/d • Start low to minimize anxiety Adjunctive BZD, beta blocker
Serotonin Selective Reuptake Inhibitors (cont) • Typical SSRI side effects: • GI distress, jitteriness, headaches, sleep disturbance, sexual disturbance • Clomipramine (Anafranil), 25-250 mg/d • Initiate with 25 mg/d • Efficacy: PDAG, PTSD, SP, OCD, GAD
Sertraline In Comorbid PTSD And Alcoholism Pre-treatment Post-treatment 140 60 40 70 IES score Standard drinks/week 20 0 0 IES Alcohol use Brady et al. J Clin Psychiatry. 1995;56:502.
Discontinuation of Treatment for Anxiety Disorders • Withdrawal/rebound more common with Bzd than other anxiolytic treatment • Relapse: a significant problem across treatments. Many patients require maintenance therapy • Bzd abuse is rare in non-predisposed individuals • Clinical decision: balance comfort/compliance/ comorbidity during maintenance treatment with discontinuation-associated difficulties
Strategies for Anxiolytic Discontinuation • Slow taper • Switch to longer-acting agent for taper • Cognitive-Behavioral therapy • Adjunctive • Antidepressant • Anticonvulsant • ?clonidine, ?beta blockers, ? buspirone
Serotonin-Norepinephrine Reuptake Inhibitor • Venlafaxine-XR (Effexor-XR) 75-300 mg/d • Initiate with 37.5 mg/d • Indicated for GAD; effective for panic disorder, social phobia, PTSD, OCD • Typical side effects • GI distress, jitteriness, headaches, sexual disturbance
Atypical Antidepressants • Nefazadone (300-500 mg/d) • 5-HT reuptake inhibitor • 5-HT2 antagonist • Initiate with 50 mg bid • Mirtazapine • Limited experience to date in anxiety disorders
Atypical Antidepressants (cont.) • Bupropion • Based on limited data, considered less effective for panic and other anxiety disorders, but reports suggestive of efficacy for • panic disorder • social anxiety disorder • PTSD • Trazodone • Based on limited data, considered less effective for panic and other anxiety disorders
Tricyclic Antidepressants • Imipramine (Tofranil) • Nortriptyline (Pamelor) • Desipramine (Norpramin) • Amitriptyline (Elavil) • Doxepin (Sinequan) • Effective in anxiety with or without comorbid depression • Recommended dosage 2.25 mg/kg/d Imipramine or its equivalent for panic • Initial anxiety worsening (Initiate with “test” dose, e.g. 10 mg/d IMI)
Tricyclic Antidepressants (cont) • Typical TCA side effects • anticholinergic effects (dry mouth, blurred vision, constipation) • orthostatic hypotension • cardiac conduction disturbance • weight gain • sexual dysfunction • Lethal in overdose • Weight gain and sedation often become increasingly problematic over time • Efficacy: PDAG, GAD, PTSD
Monoamine Oxidase Inhibitors • Phenelzine (Nardil) 45-90 mg/d • Tranylcypromine (Parnate) 30-60 mg/d • Isocarboxacid (Marplan) 10-30 mg/d • Initial worsening of anxiety is unusual • Side effects: light-headedness, neurological symptoms, weight gain, sexual dysfunction, edema • Dietary restrictions/Hypertensive crisis; “cheese reaction” • Risk of lethal overdose and toxicity • Generally reserved for refractory cases • Efficacy: PDAG, SP, OCD, PTSD
Benzodiazepines • Potency was considered critical determinant of anti-panic efficacy • Alprazolam (Xanax) • Clonazepam (Klonopin) • +/- Lorazepam (Ativan) • But comparable doses of diazepam as effective as alprazolam • All benzodiazepines effective for generalized anxiety
Potential Benefits of Benzodiazepine Therapy • Effective • Short latency of therapeutic onset • Well tolerated • Rapid dose adjustment feasible • Can be used “prn” for situational anxiety
Potential Drawbacks of Benzodiazepine Therapy • Initial sedation • Discontinuation difficulties • Potential for abuse in substance abusers • Not effective for comorbid depression
Alprazolam Effective as AD in panic Advantages: rapid onset of effect, lacks typical AD side effects Disadvantages: short duration of effect (i.e., multiple dosing, interdose rebound), discontinuation syndromes, early relapse, abuse potential, disinhibition Dosing: anticipate initial sedation (tachyphylaxis usually develops). Range: 2-10 mg/d (4-6 mg/d usual) (QID dosing)
Clonazepam • Labeled as anticonvulsant • As effective as alprazolam for panic; issue of potency for anti-panic efficacy • Advantages: Pharmacokinetic: longer duration of effect results in less frequent dosing, interdose symptoms, early relapse, or acute withdrawal symptoms. Slower onset of effect diminishes abuse potential • Disadvantages: Depression not more frequent than with other Bzd”s; disinhibition, headaches • Dosing: anticipate initial sedation (initiate at 0.25-0.5 mg qhs) • Range: 1-5 mg/d (BID dosing)
Combining Antidepressantswith Benzodiazepines • Provides rapid anxiolysis during antidepressant lag • Decreases early anxiety associated with initiation of antidepressant • Treats residual anxiety wtih antidepressant treatment • Prevents and treats depression on benzodiazepines
† * * * * Clonazepam Taper Phase * Together the Clonazepam groups differ from the Placebo group at p< .05 † Clonazepam groups differ from each other at p<.05 Pollack, et al 2001
Buspirone • Non-benzodiazepine anxiolytic • Non-sedating, muscle relaxant, anticonvulsant • Effects on serotonin and dopamine receptors • Indicated for GAD; weak antidepressant effects • Useful as SSRI augmentation for panic, social phobia, depression, sexual dysfunction • Dosing: 30-60 mg/d
Beta Blockers • Decrease autonomic arousal • May be useful as adjunct for somatic symptoms of panic and GAD but not as primary treatment • Useful for non-generalized social phobia, performance anxiety subtype • Propranolol 10-60 mg/d; Atenolol 50-150 mg/d
Anticonvulsants • Valproate and gabapentin effective for non-ictal panic • Gabapentin effective for social phobia • Gabapentin (600-5400 mg/d) used as alternative to benzodiazepine • Valproate, Carbamazepine, Gabapentin, Topiramate and Lamotrigine for PTSD
Strategies for Refractory Anxiety Disorder • Maximize dose • Combine antidepressant and benzodiazepine • Administer cognitive-behavioral therapy • Attend to psychosocial issues .
Augmentation Anticonvulsants Gabapentin Valproate Topiramate Beta blocker Buspirone Clonidine/Guanfacine Pindolol Dopaminergic agonists (e.g., Ropinirole) for social phobia Cyproheptadine Combined SSRI/TCA Alternative antidepressant Clomipramine MAOI Other Inositol Kava-kava Atypical neuroleptics Strategies for Refractory Anxiety Disorders
Cognitive-Behavioral Therapy for Anxiety Disorders • CBT useful alone or in combination with medication for • Refractory symptoms • Persistent cognitive factors, behavioral patterns and anxiety sensitivity • Comorbid conditions • Early intervention for PTSD prophylaxis • CBT may be provided by therapist or self-administered (TherapyWorks manuals 800-228-0752///http://www.psychcorp.com) • CBT may facilitate medication discontinuation .
Continuation Phase Outcome with Sertraline Treatment of PTSD Based on Acute Phase Response Category Acute PhaseResponder Status Continuation PhaseResponder Status Sustained Response Lost response Converted to responder Acute PhaseNon-responders Continued non-response Responder = > 30% decrease CAPS and CGI-S = 1 or 2 Londborg et al. J Clin Psychiatry, in press.
Long-Term Treatment Of GAD • Need to treat long-term • Full relapse in approximately 25% of patients 1 month after stopping treatment • 60%-80% relapse within 1st year after stopping treatment Hales et al. J Clin Psychiatry. 1997;58(suppl 3):76. Rickels et al. J Clin Psychopharmacol. 1990;10(3 suppl):101S.
Effect Of Venlafaxine On TotalHAM-A Scores 0 Placebo (N=123) -2 Venlafaxine XR (N=115) -4 -6 Change In Mean HAM-A Total Score -8 -10 -12 -14 -16 -18 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 Week Of Treatment P<.001 for venlafaxine XR vs placebo for all study weeks except week 1 (.003), week 4 (.002), and week 20 (.007) Venlafaxine XR doses: 75 to 225 mg/d. Gelenberg et al. JAMA. 2000;283:3082.
Placebo (N=274) Paroxetine 20-50 mg(N=599 responders) * * Paroxetine (N=285) * * * * Paroxetine Long-Term GAD Treatment % Remission Phase I: Single-Blind Phase II: Double-Blind 80 70 Randomization 60 Patients(%) 50 40 30 20 10 0 1 16 2 3 4 6 8 12 20 24 28 32 Week * P<.01 vs placebo. Remission = HAM-A 7; LOCF dataset. GlaxoSmithKline data on file, 2001.
Discontinuation of Treatment for Anxiety Disorders • Withdrawal/rebound more common with Bzd than other anxiolytic treatment • Relapse: a significant problem across treatments. Many patients require maintenance therapy • Bzd abuse is rare in non-predisposed individuals • Clinical decision: balance comfort/compliance/ comorbidity during maintenance treatment with discontinuation-associated difficulties
Strategies for Anxiolytic Discontinuation • Slow taper • Switch to longer-acting agent for taper • Cognitive-Behavioral therapy • Adjunctive • Antidepressant • Anticonvulsant • ?clonidine, ?beta blockers, ? buspirone