Informatics Solutions in the Current System
This presentation by Petr Jarolim, Director of Clinical Chemistry at Brigham and Women's Hospital, focuses on the role of informatics in improving clinical laboratory utilization. It discusses key initiatives aimed at enhancing patient safety, reducing medication errors, and implementing evidence-based medicine. By leveraging information systems, decision support tools, and monitoring strategies, healthcare professionals can optimize quality and efficiency in laboratory services. The session also addresses the challenges of traditional guidelines and highlights the advantages of computerized solutions in clinical decision-making.

Informatics Solutions in the Current System
E N D
Presentation Transcript
Informatics Solutions in the Current System Petr Jarolim Director, Clinical Chemistry, Laboratory Control, And Ambulatory Care Center Clinical Laboratories Brigham and Women’s Hospital Assistant Professor of Pathology Harvard Medical School
TDM: What Does That M Stand for? • Monitoring? • Management?
TDM: What Does That M Stand for? Management!
Partners 2003 Signature Initiatives (1) investing in quality and utilization infrastructure (2) enhancing patient safety by reducing medication errors system-wide (3) enhancing uniform high-quality by measuring performance to benchmark for selected inpatient and outpatient conditions
Partners 2003 Signature Initiatives (Continued) (4) expanding disease management programs by supporting activities for certain patients with chronic illnesses (5) improving cost-effectiveness through managing utilization trends and analysis of variance
1. Quality and Utilization Infrastructure • Information system (IS) infrastructure • Computerized provider order entry (CPOE) • Electronic medical record (EMR, LMR)
2. Enhancing Patient Safety by Reducing Medical Errors • CPOE • Decision support • EMR • Bar coding • Smart pumps
3. Uniform Quality • Evidence-based medicine • JCAHO – process and outcome measures • State initiatives and voluntary oversight groups • Measuring, feeding information back, sharing best practices, re-measuring, looking for improvements
“Evidence-based” Medicine • EBM is a set of skills which allow critical appraisal of the literature • JAMA, 1993;270:2093-2095 • Evidence is often gray, decisions black/white • Emphasis on literature more than opinion • Can help physicians make decisions to provide optimal patient care
5. Trend Management • Pharmaceuticals • High-cost tests • Radiology • Laboratory tests
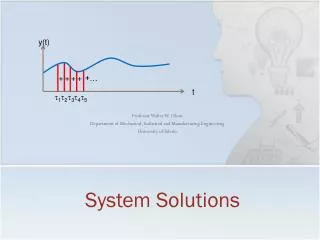
Goals • Discuss how information systems can be used to improve use of clinical laboratory • Quality • Efficiency • Specific examples • Laboratory utilization • Therapeutic drug management
Reengineering Medicine:The Role of IS • Could be changed by providing external aids • Linking medical knowledge and patient-specific data • Identifying options, helping with decisions • Without such tools, experts • Overlook available knowledge • Don’t sufficiently account for uniqueness
Why Not Rely on Experts? “The telephone is an amazing invention, but who would ever want to use one of them?” • President Rutherford B. Hayes, 1876 “The Japanese auto industry isn’t likely to carve out a big slice of the U.S. market.” • Business Week, 1968 “There is no reason for any individual to have a computer in their home.” • President, Digital Equipment Corp, 1977 From “The Experts Speak,” Cerf and Navasky, Pantheon Books, 1984
Principles of Changing Physician Behavior • Changing behavior is hard • “It’s easier to predict rain than to get people to carry umbrellas” (Lee Goldman) • Education and feedback are most likely to succeed • Feedback is most likely to influence decision-making if it is delivered as closely as possible to the time of the decision • Ideal to deliver at the time the decision is being made
Types of Decision Support • Passive display of information • Alerts and reminders • Context-specific steering • Guidelines Note: • All above can be patient-specific or not
Guidelines and Algorithms Can improve care BUT • Hard to remember • Hard to find when needed • Sometimes providers forget/don’t know about availability • Must be used by many providers • Dissemination slow • Some central control necessary
Problems With Paper Guidelines/Protocols • Paper not findable at decision time • Contain ambiguous words • No way to follow how/whether people are using or why they don’t use it • No easy way to get feedback to developers • Iterative refinement is hard
Advantages of Computerized Guidelines • Facilitate memory, always findable • Immediately generalizable to all patients, providers • Possible to point providers to them • Facilitate central control • Allow measurement of outcomes • Easy to get feedback to developers, allow iterative refinement
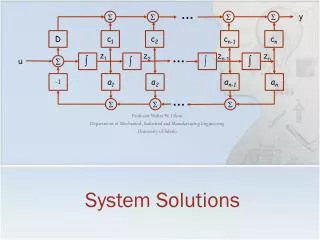
Architecture of the Event Monitor Applications (new data) Patient database Applications (new data) Applications (new data) page, email, write to file (real time message) Annun-ciators Inference engine (decisions) Coverage List Rule editor Knowledge base
Interventions to Improve Laboratory Utilization • Charge display • Redundant test reminders • Structured ordering with counterdetailing • Guidelines • Critical laboratory results paging
Redundant Reminders - Frequency Guidelines • Urine and sputum cultures, UA, Chem-20 • >1/day • Digoxin, aminophylline • >1/day, suppress if last result abnormal • Aminoglycosides, vancomycin • >2/day • Fibrin split products • >Q8h
Redundant Reminder Study • 5700 intervention admissions, 5886 control • 939 apparently redundant tests ordered • Tests cancelled 69% of time in intervention group • Redundant tests performed: Intervention group 27% Control group 51% p<0.001
Evaluating the Appropriateness of Digoxin Level Monitoring 1998 – Digoxin levels accounted for 21% of all TDM Aim of the study: • To develop appropriate criteria for measuring digoxin levels in both inpatients and outpatients • To use these criteria to evaluate the appropriateness of digoxin determinations • To determine how often levels with an inappropriate indication generated clinically important results
Digoxin Level Monitoring –Results for Inpatients - 16% of orders were appropriate - Only 14% had results > 1.7 ng/ml, none of these levels resulted in an important change in therapy and no patient had a toxic reaction - Daily routine monitoring accounted for 78% of inappropriate levels Canas et al, Arch Intern Med 1999;159:363-8
Digoxin Level Monitoring -Results for Outpatients - 52% of orders were appropriate - Only 6% had results > 1.7 ng/ml, one result led to a change in therapy, none of the patients were believed to experience a toxic reaction - Among the inappropriate levels, 87% patients underwent early routine monitoring before a steady state was achieved Canas et al, Arch Intern Med 1999;159:363-8
Errors in Outpatient Amiodarone Monitoring - Goals • To develop a model of medication monitoring • To use the model to determine at what medication monitoring stages most errors occur • To assess the incidence and preventability of ADEs associated with monitoring errors Stelfox T et al., BWH, 2002
Amiodarone • Numerous organ toxicities: • Liver • Lung • Thyroid • Heart • Skin • High incidence of ADEs: 34% - 93% • Toxicities dependent on dose and duration of therapy
Initiation of Therapy • Prescription for amiodarone • Baseline evaluation (< 2 months of first prescription): • Electrolytes and creatinine • Pulmonary function tests (PFTs) including CO diffusion capacity
Surveillance • Liver enzymes every 6 mo. • Thyroid tests (TSH or free T4) every 6 mo. • Electrocardiogram (ECG) every 12 mo. • Chest x-ray or PFTs every 12 mo.
Surveillance Response (Within 2 Months of An Abnormal Result) • If liver enzymes >2 times normal then • Any hepatic test, provider visit or dose change • If TSH abnormal (<0.5 or >5.0) then • Any thyroid test, provider visit, dose change or thyroid therapy • If possible pulmonary toxicity then • Any pulmonary test, provider visit, dose change or oral corticosteroid prescription • If ECG with HR < 50, long QTc or PR>0.2 then • Any cardiac test, provider visit or dose change
Follow-up Visit • Provider visit every 3 months during the first year and subsequently every 6 months
Errors in Outpatient Amiodarone Monitoring - Conclusions • 9% received recommended monitoring • Errors identified at all monitoring stages • Study highlights the challenges of outpatient monitoring • Some amiodarone-related ADEs are associated with monitoring errors Stelfox T et al., BWH, 2002
Appropriateness of Antiepileptic Drug Level Monitoring Drug % Appropriate Phenytoin 29 Carbamazepine 26 Phenobarbital 28 Valproic acid 26 Schoenenberger RA et al.: JAMA 1995;274:1622-6
A Computer-Based Intervention for Improving the Appropriateness of Antiepileptic Drug Monitoring Design and implementation of 2 automated computerized screens for use at the time of AED test order entry Aim: Improve appropriateness by reminding physicians when a potentially redundant test was ordered and providing common indications for monitoring AED Chen P et al., Am J Clin Pathol 2003;119:432-438
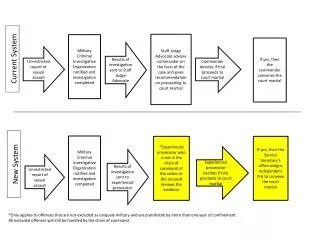
Algorithm for computerized interventions Inpatient AED test orders placed via computerized order entry Potentially redundant tests Non-redundant tests Orders not canceled Automated reminder screen Education and indications screen Test indication selected by physician Orders cancelled by physician Orders cancelled by physician Test orders completed
Algorithm for computerized interventions Inpatient AED test orders placed via computerized order entry Potentially redundant tests Non-redundant tests Orders not canceled Automated reminder screen Education and indications screen Test indication selected by physician Orders cancelled by physician Orders cancelled by physician Test orders completed
A Potentially Redundant Test Reminder Potential Redundant Lab Redundant Order: PHENOBARBITAL LEVEL: NEXT AVAILABLE; 1)PHENOBARBITAL LEVEL (05/24 1:15P) RESULTS: PHENO:pend, This reminder may be ignored if drug toxicity is suspected or if seizures have recurred CONTACT .... IF YOU HAVE QUESTIONS [X]C Cancel order(s) [ ]P Proceed with order(s)
Algorithm for computerized interventions Inpatient AED test orders placed via computerized order entry Potentially redundant tests Non-redundant tests Orders not canceled Automated reminder screen Education and indications screen Test indication selected by physician Orders cancelled by physician Orders cancelled by physician Test orders completed
Drug-Specific Information on AED orders INDICATIONS FOR PHENOBARBITAL DRUG LEVEL Please enter the indication for ordering this level [ ]A Recent seizure [ ]B Suspected toxicity (sedation, depression) [ ]C Baseline determination (>20 days after start of therapy) [ ]D New determination (>20 days after change in therapy) [ ]E Additional interacting drug added (>20 days ago) [ ]F Recent change in liver/GI function [ ]O Other 70% of phenobarbital levels done at BWH were found to be inappropriate in a recent study. A steady state is not reached until 20 days after initiation of change in therapy. Daily determination is almost never indicated. The test may not be indicated if it is not being done for one of the reasons listed above
Indication for Ordering Inpatient Serum AED Levels Indications for ordering Non-redundant Appearing Redundant (n = 409) (n=305) New or baseline serum level 159 (38.9%) 82 (26.9%) Recent seizure 121 (29.6%) 72 (23.6%) Suspected toxic effects 52 (12.7%) 32 (10.5%) Addition of interacting drugs 12 (2.9%) 8 (2.6%) Change in liver or GI function 15 (3.7%) 8 (2.6%) Other 24 (5.9%) 26 (8.5%) Orders canceled at prompt 26 (6.4%) 77 (25.2%)
Effect of Computer-based Intervention on Phenytoin Monitoring