GLGi: Cystic Fibrosis
330 likes | 688 Vues
GLGi: Cystic Fibrosis . September 18, 2007 San Francisco. Council Member Biography:

GLGi: Cystic Fibrosis
E N D
Presentation Transcript
GLGi: Cystic Fibrosis September 18, 2007 San Francisco
Council Member Biography: • Carlos Milla, MD, is an Associate Professor in the Department of Pediatrics at Stanford University. Prior he was the Director of Minnesota Cystic Fibrosis Center at the University of Minnesota. Dr Milla is trained in epidemiology and is on the faculty of the Center for Excellence in Pulmonary Biology. He has extensive experience in treatment of childhood respiratory illnesses and has an active research program in cystic fibrosis. Dr. Milla’s main areas of interest include inflammatory responses that lead to airway disease. He has actively participated in multiple cystic fibrosis-related clinical studies, and has accumulated extensive experience on implementation and conduct of clinical trials. Dr. Milla is familiar with different regulatory issues involved in the conduct of clinical studies, particularly those related to development of new therapies. © 2007 Gerson Lehrman Group Inc., All Rights Reserved
Table of Contents • Review the features of Cystic Fibrosis • Review the current treatment paradigm and available therapies • Review the outstanding therapeutic needs in this patient population • Review therapies under development and potential impact © 2007 Gerson Lehrman Group Inc., All Rights Reserved
Gerson Lehrman Group Contacts HEALTHCARE & BIOMEDICAL (HC) Craig Cinquina, PhD Vice President, Healthcare Gerson Lehrman Group + 1 212 984 3640 ccinquina@glgroup.com HEALTHCARE & BIOMEDICAL (HC) Tasha Bengoechea, PhD Senior Research Manager, Healthcare Gerson Lehrman Group + 1 415 343 6371 tbengoechea@glgroup.com Christine Ruane Senior Product Manager Gerson Lehrman Group 850 Third Avenue, 9th Floor New York, NY 10022 + 1 212 984 8505 cruane@glgroup.com
About GLG Institute GLG Institute (GLGiSM) is a professional organization focused on educating business and investment professionals through in-person meetings. It is designed to revolutionize the professional education market by putting the power of programming into the hands of the GLG community. GLGi hosts hundreds of Seminars worldwide each year. GLGi clients receive two seats to all Seminars in all Practice Areas. GLGi’s website enables clients to: • Propose Seminar topics, agenda items and locations • View and RSVP to scheduled and proposed Seminars • Receive a daily briefing with new posts on your favorite tickers, subject areas and from trusted Council Members • Share Seminar details with colleagues or friends
IMPORTANT GLG INSTITUTE DISCLAIMER – By making contact with this/these Council Members and participating in this event, you specifically acknowledge, understand and agree that you must not seek out material non-public or confidential information from Council Members. You understand and agree that the information and material provided by Council Members is provided for your own insight and educational purposes and may not be redistributed or displayed in any form without the prior written consent of Gerson Lehrman Group. You agree to keep the material provided by Council Members for this event and the business information of Gerson Lehrman Group, including information about Council Members, confidential until such information becomes known to the public generally and except to the extent that disclosure may be required by law, regulation or legal process. You must respect any agreements they may have and understand the Council Members may be constrained by obligations or agreements in their ability to consult on certain topics and answer certain questions. Please note that Council Members do not provide investment advice, nor do they provide professional opinions. Council Members who are lawyers do not provide legal advice and no attorney-client relationship is established from their participation in this project. You acknowledge and agree that Gerson Lehrman Group does not screen and is not responsible for the content of materials produced by Council Members. You understand and agree that you will not hold Council Members or Gerson Lehrman Group liable for the accuracy or completeness of the information provided to you by the Council Members. You acknowledge and agree that Gerson Lehrman Group shall have no liability whatsoever arising from your attendance at the event or the actions or omissions of Council Members including, but not limited to claims by third parties relating to the actions or omissions of Council Members, and you agree to release Gerson Lehrman Group from any and all claims for lost profits and liabilities that result from your participation in this event or the information provided by Council Members, regardless of whether or not such liability arises is based in tort, contract, strict liability or otherwise. You acknowledge and agree that Gerson Lehrman Group shall not be liable for any incidental, consequential, punitive or special damages, or any other indirect damages, even if advised of the possibility of such damages arising from your attendance at the event or use of the information provided at this event.
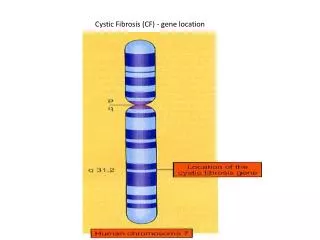
Cystic Fibrosis • Multisystemic process with defective ion transport across mucosal surfaces. • Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) protein (1480 aa’s) is affected. • Gene in chromosome 7 (250 kb). • Lung Manifestations: Chronic inflammatory process.
US Incidence of CF by Race • White 1:3,000 • Black 1:15,000 • Hispanic 1:9,500 • Native 1:10,000 • Asian 1:30,000 • Global 1:4,000
US Carriage Rate by Race • White 1:25 • Black 1:60 • Hispanic 1:45 • Native 1:50 • Asian 1:90 • Global 1:30
The Evolution of Survival in CF:1936 - 2005 36.8 Median Survival Age (Years)
CF Manifestations Obstructive Lung Disease Bronchiectasis Chronic Infection Chronic Sinusitis Nasal Polyposis Pancreatic Insufficiency Cholestasis Cirrhosis Male Infertility Bowel Obstruction Malnutrition High Cl- in Sweat Adapted from Welsh and Smith. Sci Am. 1995;273:52-59.
Pathogenesis of lung disease in cystic fibrosis Defective CF gene Defective/deficient CFTR Bronchial obstruction Infection Inflammation Abnormal airway surface milieu Bronchiectasis Davis & Konstan, AJRCCM 2000
CFTR Gene Mutation Defective CFTR Deranged Airway Environment
Airway Surface Fluid Volume is Decreased in CF Cl- Na+ Cl- Na+ Normal CF
Essentials of Medical Management in CF • Optimize airway clearance • Optimize pancreatic enzyme replacement and nutritional status • Minimize airway injury • Respiratory illnesses • Environmental factors • Treat aggressively symptomatic episodes • Judicious use of Antibiotics • Evolving trend of more aggressive Rx • Balance micro + clinical benefit with safety/burden of care • Role of prophylactic antibiotics debatable (S. aureus)
“Prophylactic” Therapeutic Approach • Establish therapeutic intervention in pre-symptomatic stage • Early changes are reversible, however once bronchiectasis develops, damage is irreversible • Best treatment is prevention, daily program ofairway clearance is best preventative measure • Consistent routine that is followed rigorously is necessary to prevent or delay any progression • Chronic suppressive antibiotics if infection present • Role of antiinflammatory therapy has been established, but side effect profile less than optimal
Airway Clearance • Chest physiotherapy by manual percussion and postural drainage ‘Gold standard’ • An array of alternative techniques available • 20 – 30 minutes per session • 2 sessions per day, increase during symptomatic episodes
Aerosol Therapy • Bronchodilators Albuterol Ipratropium • Mucolytics N-Acetylcysteine Hypertonic Saline rH-DNase • Antibiotics Tobramycin (Colistin, Aztreonam) • Anti-inflammatory Budenoside, fluticasone, others Na Cromoglycate (Azithromycin)
The Patient Perspective: Treatment Burden • Stenzel • Photo by Derek Powazek http://www.thebreathingroom.org/
PTC Vertex Inspire Bronchitol RespirTech Gilead Transave Bayer KaloBios NAC Current treatments of cystic fibrosis lung disease Defective CF gene Defective/deficient CFTR Abnormal airway surface milieu Hypertonic saline Airway clearance rhDNase Bronchial obstruction Systemic antibiotics Inhaled antibiotics Azithromycin Infection Corticosteroids Ibuprofen Inflammation lung transplantation Bronchiectasis Adapted from Davis P, AJRCCM 2000
PTC Therapeutics: PTC 124 for Stop Mutations defects • Drug well tolerated • 18 out of 42 patients from the two studies had responded with a change of at least -5 mV in chloride secretion TEPD • 15 out of 42 patients had chloride secretion TEPD values higher than -5 mV • Mild, statistically significant reductions in blood neutrophil counts • Mild improvements in Liver enzymes 2006 NACFC
Inspire: Denufosol (P2Y2 Agonist) Deterding RR et al, AJRCCM 2007
Gilead: Aztreonam Lysinate for Inhalation McKoy K et al. 30th European CF Conference, June 2007
RespirTech: HFCWO Vest Kempainen R et al, Chest, in press
N-Acetyl Cysteine: High-Dose effects • Increases Glutathione in blood Neutrophils • Decreases Sputum Neutrophil count and sputum elastase activity • Decreases IL-8 in Sputum • Statistically significant decrease in incidence of pulmonary exacerbations (22% vs 78%) and number of episodes per subject. • Proceeding to larger Phase III confirmatory study Tirouvanziam R et al PNAS 2006 Conrad C, 2007 CFTDN meeting
Pancreatic Enzyme Replacement Therapy (PERT) Studies • Pancreatic enzyme preparations of porcine or bovine origin were available in the United States for treatment of exocrine pancreatic insufficiency (PI) prior to the enactment of the FDA. • Outbreak of severe Colitis in the mid 90’s associated with high dose products • In the late 90’s the FDA determined that PERT did not meet the requirements of an OTC preparation and made a decision that all PERT products must go through an NDA process • Guidance for Industry drafted and all PERT manufacturers required to file NDA for their product by 2008.
Altus Pharmaceuticals: ALTU-135 PERT Borowitz et al, J Peds 2006
Altus Pharmaceuticals: ALTU-135 PERT Borowitz et al, J Peds 2006
The Cystic Fibrosis Foundation Drug Development Pipeline Approved Phase III Phase II Phase II Phase I Pre-clin. Cff.org – Sept. ‘07