Download
1 / 36
380 likes | 714 Vues
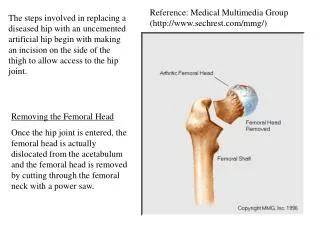
Quantifying of avascular necrosis of femoral head. The clinical problem Determining the risk of femoral head collapse in a patient with AVNFH. Step 1. Asking an answerable question.

E N D
Quantifying of avascular necrosis of femoral head The clinical problem Determining the risk of femoral head collapse in a patient with AVNFH
Step 1. Asking an answerable question • In a 36-year-old woman with a 1-year history of avascular necrosis of femoral head, what is the risk for developing femoral head collaspse( Ficat stage III)?
Quantifying the Extent of Femoral Head Involvement in Osteonecrosis • By SEBASTIAN F. CHERIAN, MD, ALAN LAORR, MD, KHALED J. SALEH, MD, MSC, FRCSC, MICHAEL A. KUSKOWSKI, PHD, ROBERT F. BAILEY, LPN, AND EDWARD Y. CHENG, MD • Investigation performed at the Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, Minnesota
Quantifying the Extent of AVNFH • There are numerous methods for quantifying the extent of osteonecrosis of the femoral head. • However, there is no consensus regarding which method is the most reliable. • The purpose of this study was to determine the reliability and prognostic accuracy of “three” commonly used methods for quantifying the extent of osteonecrosis of the femoral head.
Quantifying the Extent of AVNFH • The interobserver and intraobserver agreement was determined for each method • The ability of each method to predict the time to subchondral collapse was analyzed statistically.
Quantifying the Extent of AVNFH • Joint-preserving surgical interventions generally more successful at earlier stages of bone involvement (before the occurrence of a subchondral fracture). • The concept of quantifying femoral head involvement (important in determining prognosis) introduced by The staging system of Steinberg et al.
Quantifying the Extent of AVNFH • Subchondral fracture is the most prognostically important variable indicating progression to osteoarthritis. • Several studies have demonstrated that the size of the necrotic lesion is important in determining whether a subchondral fracture will occur • Size necrotic volume or the surface area or arc of subchondral bone affected ??
Quantifying the Extent of AVNFH • Methods: • Thirty-nine hips in twenty-five patients who had stage-I or II osteonecrosis of the femoral head, according to the grading system of the Association Research Circulation Osseous, were independently examined on twoseparate occasions bythreeobservers of different specialty backgrounds and experience. • Each observer used three methods to quantify the extent of osteonecrosis of the femoral head: (1) the percentage of femoral head involvement. (2) the index of necrotic extent (3) the modified index of necrotic extent
Materaial and methods • The three raters in this study : 1. a third-year radiology resident 2. an attending staff musculoskeletal radiologist 3. an attending staff orthopaedic surgeon • The observers were blinded to both their previous evaluations and the evaluations of the other observers.
The percentage of femoral head involvement • first described in 1984 • the abnormal signal on T1-weighted images • visually estimated on the basis of serial coronal and sagittal images • according to the estimated percentage of the area involved compared with the area of the entire femoral head, were grouped into three categories, as <15%, 15% to 30%, and >30%.
The index of necrotic extent • developed by Koo and Kim in 1995 • The necrotic arc angles on the midcoronal and midsagittal images were designated A and B, respectively. • The index of necrotic extent was calculated as (A/180) × (B/180) × 100
The modified index of necrotic extent • The necrotic arc angle is measured on the image that demonstrates the maximal lesionsize in the sagittal (A) and coronal (B) planes rather than on the midcoronal and midsagittal images.
Result--- Reliability and Validity • The interobserver agreement as defined by intraclass correlation coefficients • The index of necrotic extent 0.58 (p < 0.001) for the first observation 0.70 (p < 0.001) for the second observation. • The modified index of necrotic extent 0.63 (p < 0.001) for the first observation 0.81 (p < 0.001) for the second observation. • The interobserver agreement of the percent involvement, as defined by Kendall coefficients of concordance, 0.71 (p < 0.001) for the first observation 0.79 (p < 0.001) for the second observation.
Result--- Reliability and Validity • The intraobserver agreement---nearly perfect • The index of necrotic extent 0.91 (p < 0.005) for the first rater 0.83 (p < 0.005) for the second rater, 0.93 (p < 0.005) for the third rater. • The modified index of necrotic extent 0.65 (p <0.005) for the first rater 0.88 (p < 0.005) for the second rater 0.91 (p < 0.005) for the third rater. • The percent involvement 0.90 (p < 0.005) for the first rater 0.89 (p < 0.005) for the second rater 0.88 (p <0.005) for the third rater
Result--- Prognostic Ability (1) • the percent involvement was significantly related to (log rank = 5.81, p < 0.05) the time to subchondral collapse
Result--- Prognostic Ability (2) • index of necrotic extent (log rank = 7.17, p < 0.007)
The index of necrotic extent • (A/180) × (B/180) × 100 = 40 A x B = 40 x 180 x 180 / 100 = 12960 假設 A等於 B A2 = 12960 A = = 113.8 degree 12960
Result--- Prognostic Ability (3) • modified index of necrotic extent (log rank = 4.05, p < 0.04)
Critical Appraisal • Evidence level ? • Reliability and Validity • Reproducibility • Limitation
Interobserver Agreement • Epidemiologists consider interobserver agreement of 0.6 to 0.8 to be substantial and 0.8 to 1.0 to indicate nearly perfect agreement . • With the sample size used in this study (thirty-eight hips), a correlation coefficient of 0.44 could be detected as significant at the p = 0.05 level with 80% power. • Kendall coefficients of concordance : for a noncontinuous categorical variable ( groups)
Reliability and Validity • The interobserver agreement as defined by intraclass correlation coefficients • The index of necrotic extent 0.58 (p < 0.001) for the first observation 0.70 (p < 0.001) for the second observation. • The modified index of necrotic extent 0.63 (p < 0.001) for the first observation 0.81 (p < 0.001) for the second observation. • The interobserver agreement of the percent involvement, as defined by Kendall coefficients of concordance, 0.71 (p < 0.001) for the first observation 0.79 (p < 0.001) for the second observation.
Reliability and Validity • The intraobserver agreement---nearly perfect • The index of necrotic extent 0.91 (p < 0.005) for the first rater 0.83 (p < 0.005) for the second rater, 0.93 (p < 0.005) for the third rater. • The modified index of necrotic extent 0.65 (p <0.005) for the first rater 0.88 (p < 0.005) for the second rater 0.91 (p < 0.005) for the third rater. • The percent involvement 0.90 (p < 0.005) for the first rater 0.89 (p < 0.005) for the second rater 0.88 (p <0.005) for the third rater
Limitations • Only three observers • Sample size (38 hips) • Other variables ( surgical intervention, medication, weight bearing status etc…) • Configuration of the lesions
Results • There was significantly valid agreement among the observers for all three methods (p < 0.001 for all three). • The index of necrotic extent and the percent involvement →substantial agreement among raters The modified index of necrotic extent →nearly perfect agreement • Survivorship analysis revealed prognostically significant predictors of subchondral fracture. the percent involvement (p < 0.05) index of necrotic extent (p < 0.007) modified index of necrotic extent (p < 0.04)
Conclusions • index of necrotic extent, modified index of necrotic extent, and estimation of the percentage of involvement of the femoral head are reproducible and reliable methods for quantitatively evaluating the extent of osteonecrosis of the femoral head. • Furthermore, they are clinically useful for identifying hips at greatest risk for subchondral collapse.