Download
1 / 17
200 likes | 878 Vues
Encéphalopathie hypertensive. Réunion ARCO du 10/11/05 Réanimation polyvalente La Roche sur Yon FLORENCE WASMER. Mme F. âgée de 33 ans est hospitalisée en Réanimation pour état de mal épileptique. ATCD Migraine Fausse couche en 2004

E N D
Encéphalopathie hypertensive Réunion ARCO du 10/11/05 Réanimation polyvalente La Roche sur Yon FLORENCE WASMER
Mme F. âgée de 33 ans est hospitalisée en Réanimation pour état de mal épileptique • ATCD • Migraine • Fausse couche en 2004 • Métrorragies depuis 2-3 mois en cours d’exploration (biopsie du col en attente) • Traitement habituel • Adepal
HDLM • Céphalées intenses depuis une semaine avec vomissements • Le 4/11/2005, clonies du membre supérieur droit puis de l’hémicorps droit, perte de contact, sueurs • Appel SAMU • Persistance clonies MSDt, pas de Babinsky, Glasgow 3, perte d’urine • PA à 230/160 mmHg, dextro à 2,10 g/L • PEC immédiate • Rivotril, IOT, sédation • Loxen
PL LCR clair Biochimie hématies 78/mm3 glycorachie 4.92mmol/l protéinorachie 0.41g/l Cytologie éléments 5/mm3 culture stérile NFS leucocytes 23030/mm3 Hb 13.4 g/dl plaquettes 564000/mm3 Ionogramme Na 136 mmol/l K 4.8 mmol/l Créatinémie 387 µmol/l Urée 19.9 mmol/l Aux Urgences
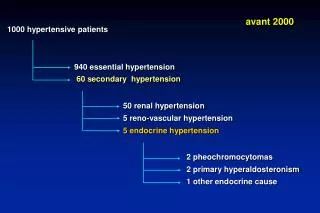
Les hypothèses évoquées • Encéphalopathie hypertensive • Méningoencéphalite herpétique • Microangiopathie thrombotique • Thrombophlébite cérébrale • Tumeur cérébrale • Etat de mal épileptique idiopathique
EEG : pas argument pour un état de mal non convulsivant , suspicion d’atteinte pontique
Diagnostic • IRM cérébrale : hypersignaux Flair du cortex pariéto-occipital gauche compatible avec une encéphalopathie aigue hypertensive • FO normal
Les hypothèses évoquées • HTA maligne avec atteinte rénale • SHU • Glomérulopathie (GEM secondaire) • Uropathie obstructive
Biologie • Hb 13.4 g/dl , haptoglobine 2.58 g/l , LDH 521 U/l, schizocytes <1% pas hémolyse • ECBU : <10000/ml leucocytes <10000/ml hématies absence de germes au direct • EPPU : protéinurie 0.34g/l 0.68g/24h 62.3% alb, 11.3% α1glob, 9.4% α2glob, 7.1% βglob, 9.9% γ
Examen morphologique • Echographie rénale: dilatation des cavités à droite et à gauche, un bassinet dilaté à gauche et non dilaté à droite
Diagnostic et traitement • Uropathie obstructive • Traitement • Montée de sondes JJ • Constatation per opératoire • Tumeur du col • Pas d’envahissement du trigone, compression extrinsèque des uretères (adénopathies lombo aortiques?) • Anatomopathologie • Carcinome infiltrant du col utérin
Evolution • Amélioration de la fonction rénale avec diminution de la créatinémie • Normalisation de la pression artérielle
Diagnostic final • Encéphalopathie hypertensive secondaire à une insuffisance rénale aigue obstructive • Carcinome épidermoide infiltrant du col