Download
1 / 22
220 likes | 322 Vues
Learn about the importance of folic acid in preventing neural tube defects, such as spina bifida and anencephaly. Discover the history, studies, and evidence supporting folic acid's role. Findings from the Medical Research Council RCT are also highlighted.

E N D
Folic Acid and Neural Tube Defects Yongling Xiao
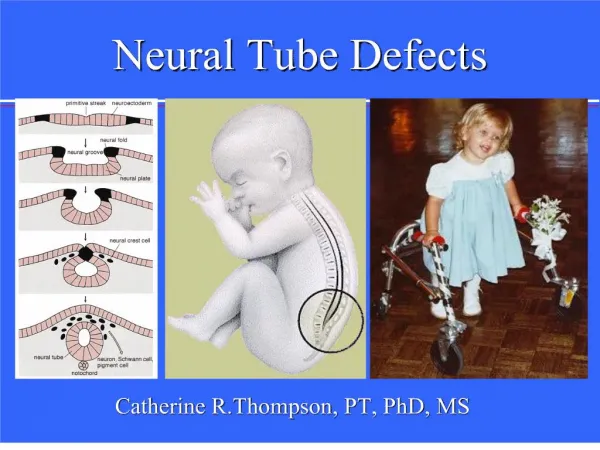
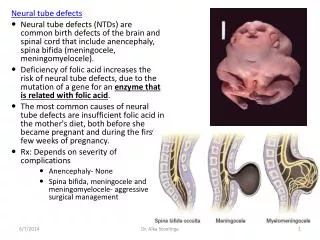
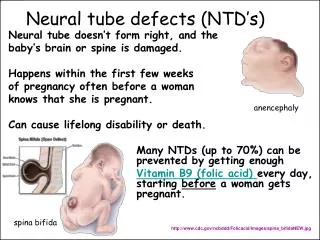
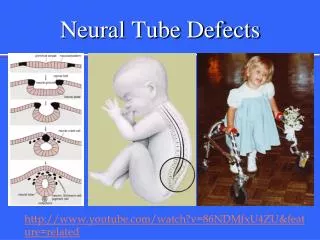
Neural Tube Defects (NTD) • NTD are birth defects of the brain and spinal cord. Normally, in human embryos, the closure of the neural tube occurs around the 30th day after fertilization. However, if something interferes and the tube fails to close properly, a NTD will occur.
Neural Tube Defects • The two most common NTD are: • Spina bifida (Latin: "split spine" ): incomplete closure of the embryonic neural tube results in an incompletely formed spinal cord during the first month of pregnancy. There is usually nerve damage that causes at least some paralysis of the legs. • Anencephaly, when the head end of the neural tube fails to close, resulting in the absence of a major portion of the brain, skull, and scalp. Babies with anencephaly are either stillborn or die shortly after birth.
Folic Acid • Folic acid (FA) is a water-soluble Vitamin B9, also called Folate. • Foods with folic acid include leafy green vegetables, fruits, dried beans, peas and nuts • Dietary supplement • Folate deficiency • In adults, anemia is a sign of advanced folate deficiency. • A deficiency of folate can occur when • need for folate is increased, • dietary intake of folate is inadequate, • body excretes (or loses) more folate than usual
First observation • Connection between FA and congenital malformations began with animal studies of aminopterin, an antimetabolite of FA, in 1949 by Nelson. • The invariable effect of aminopterin on pregnant ratswas prenatal death, but not malformations. • This outcome led Thiersch, a pathologist, to use aminopterin as a means of interrupting pregnancy in women • 12 women were given aminopterin during the 1st trimester. • Abortion occurred in only 10 /12. One of the ten and the other two had offspring possessing various malformations. • For the first time, human embryos were shown to be capable of being malformed by chemical substances.
Smithells’ study • In 1964, Smithells et al. conducted a study in Liverpool to investigate a possible relationship between fetal malformations & defective folate metabolism in mother • Of 98 mothers of severe malformed (principally of the central nervous system) infants in 1964, 54 were matched satisfactorily with controls, those who gave a normal infant in the same hospital and were selected with respect to age, parity and the time of conception and gestation. • A FIGLU excretion test was used to test FA
Smithells’ study • A significant relationship between malformation of the fetus and defective folate metabolism in the mother. • However, • The results were based on the investigation of a metabolic defect present in late pregnancy, thus, did not indicate necessarily that such a defect was present at the time of embryogenesis. • A positive FIGLU test may indicate defective metabolism rather than deficient intake of folate.
Evidence • A retrospective study of FA and NTD occurrence conducted as part of Metropolitan Atlanta Birth Defects Program found that multivitamin use was twice as great in control women, with infants without malformation or with other non-NTD malformations, as in case women who had NTD births in 1968 through 1980, with the respective estimated overall NTD risk being 0.4. • The Boston prospective study performed in 1984 to 1987 showed that the frequency of offspring with NTD of those who replied negatively of vitamin use was 3.0 per 1000 and replying positively 0.9 per 1000, a reduction of 70%.
Evidence • Contradictive finding in a NIH study: no significant difference was found in the rate of use of multivitamin between case group (women with infants or fetuses with a NTD diagnosed in 1985 – 1987) and 2 control groups (women with normal offspring and another with non-NTD major malformations). • In 1980, a multicenter intervention project undertaken in Leeds, reported that 1/178 offspring of the treated (i.e. a commercial multivitamin) women had a NTD, whereas 13/260 offspring of the control (already pregnant or refused ) women had a NTD (0.6% vs 5.0%).
Medical Research Council RCT • The British double-blind randomized trial was launched in July, 1983, and continued till 1991 • 33 centers ( 17 in UK and 16 in other countries: Hungary, Israel, Australia, Canada, USSR and France) • 1817 women at high risk of having a pregnancy with a NTD (because of a previous affected pregnancy) were allocated to one of the four groups. Group Folic Acid(4mg/day) Other vitamins A yes no B yes yes C no no D no yes
Medical Research Council RCT • Relative risk for the women allocated to take FA was 0.28 compared with the control groups (72% of the NTD were prevented) • No indication that the vitamins other than FA had any preventive effect nor that they enhanced the effect of FA • MRC trial study has established the specific role of folic acid in the prevention of NTD. • In MRC trial, FA supplementation had been shown to reduce the NTD recurrence rate, whether the same could be achieved for first time occurrence of these abnormalities?
Another Randomized Trial • The results of Hungarian RCT was reported in 1992 • To test the efficacy of periconceptional multivitamin supplementation in reducing the incidence of a first occurrence of NTD. • Women planning a pregnancy were randomly assigned to receive a single tablet of a vitamin supplement (containing 12 vitamins, including 0.8 mg of FA) or a placebo supplement daily for at least one month before conception • Significant difference was found: 6 cases of NTD in the placebo group (n=2052), as compared with 0 in the vitamin-supplement group (n=2104) (P = 0.029)
Folic Acid Fortification (FAF) • In 1992, U.S. Public Health Service recommended that “All women of childbearing age in the United States who are capable of becoming pregnant should consume 0.4 mg of folic acid per day for the purpose of reducing their risk of having a pregnancy affected with spina bifida or other NTDs.” • However, a survey indicated that only 29% of US women were following this recommendation.
Folic Acid Fortification (FAF) • In a further effort to reduce the occurrence of folate-preventable NTDs, the US FDA authorized the addition of FA to enriched grain products at a level of 140µg/100g flour in March 1996 and made compliance mandatory by January 1998. • The Canadian milling industry started fortification early in 1997, to meet the US requirements for imported flour. On November 11, 1998, fortification with FA of all types of white flour, enriched pasta, and cornmeal became mandatory in Canada.
Evaluation of Folic Acid Fortification • A study was conducted in Canada • To assess changes in the prevalence of NTD associated with food fortification with FA throughout Canada. • To test the hypothesis that the magnitude of the effect of FA fortification would vary with the baseline rate of the defect • Study population included live births, stillbirths, and terminations of pregnancies because of fetal anomalies among women residing in seven Canadian provinces from 1993 to 2002 • 2446 subjects with NTD were recorded among 1.9 million births • Study periods: • Prefortification: Jan. 1, 1993, to Sept. 30, 1997 • Partial-fortification: Oct.1, 1997 to Mar.31, 2000 • Full-fortification: April 1, 2000 to Dec. 31, 2002
Evaluation of Folic Acid Fortification • The prevalence of NTD decreased from 1.58 per 1000 births before fortification to 0.86 per 1000 births during the full-fortification period, a 46% reduction.
Evaluation of Folic Acid Fortification • The magnitude of the decrease was proportional to the prefortification baseline rate in each province, and geographical differences almost disappeared after fortification began.
Evaluation of Folic Acid Fortification • Conclusions: • Food fortification with FA was associated with a significant reduction in the rate of NTD in Canada. • The decrease was greatest in areas in which the baseline rate was high.
Concerns about possible adverse effects of Folic Acid Fortafication • Possible adverse effects due to FA: • Masking B12 deficiency and consequent neurologic damage • Intake in children • Decreased natural killer cell activity • Cancer promotion • The evidence available to date does not support the conclusion that foods fortified with FA cause harm • However, the possibility that higher FA intake may pose a risk to the general population must be taken into consideration seriously.