Download
1 / 1
10 likes | 208 Vues
OPTIONAL LOGO HERE. NEONATAL OUTCOME IN CASES OF PREGNANCY INDUCED HYPERTENSION WITH HYPERURICAEMIA Samra Ayub 1 , Ayesha Basharat 1 , Asma Tanvir Usmani 1 , Waqas Ayub 2 1 Benazir Bhutto Hospital, Rawalpindi, Pakistan, 2 Rawalpindi Medical College, Rawalpindi, Pakistan. OPTIONAL LOGO HERE.

E N D
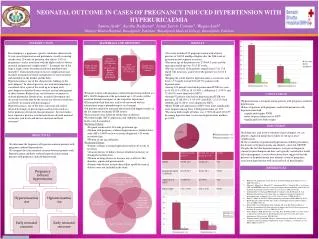
OPTIONALLOGO HERE NEONATAL OUTCOME IN CASES OF PREGNANCY INDUCED HYPERTENSION WITH HYPERURICAEMIA Samra Ayub1, Ayesha Basharat1, Asma Tanvir Usmani1, Waqas Ayub2 1Benazir Bhutto Hospital, Rawalpindi, Pakistan, 2Rawalpindi Medical College, Rawalpindi, Pakistan OPTIONALLOGO HERE RESULTS INTRODUCTION MATERIALS AND METHODS Preeclampsia is a pregnancy specific syndrome characterised by new onset hypertension and proteinuria, usually occurring usually after 20 weeks of gestation, that affects 2-8% of pregnancies1 and is associated with the highest risk of adverse maternal and perinatal complications2,3. It remains one of the largest single causes of maternal and fetal morbidity and mortality4. Clinical prediction of disease complications may facilitate instigation of timely management to avert mortality and morbidity in the mother and the baby. Hyperuricaemia is one of the characteristic findings in the preeclampsia5. In clinical practice, uric acid determination is considered to be a part of the work up in women with preeclampsia to monitor disease severity and aid management of these women. Reduced uric acid clearance secondary to reduced glomerular filtration rate, increased absorption and decreased secretion may be the reasons for elevated serum uric acid levels in women with preeclampsia6. Hyperuricaemia is one of the most consistent and earliest detectable changes in preeclampsia and has been cited as a better predictor of fetal risk than proteinuria7. Several studies have reported a positive correlation between elevated maternal serum uric acid levels and adverse maternal and fetal outcomes8. • Our study included 150 pregnant women with a blood pressure of 140/90 mmHg or higher after the 20th week of gestation on two separate occasions. • The mean age of the patients was 27.48+4.3 years and the mean gestational age was 352.85 weeks. • The uric acid level of the patients ranged from 2.5 to 12.8 mg/dl. The mean uric acid level of the patients was 6.31.8 mg/dl. • Keeping the cutoff limit for hyperuricemia as serum uric acid level > 5.5 mg/dl; we had 103 (68.7%) patients with hyperuricemia. • Among 103 patients who had hyperuricemia IUGR was seen in 99 (96.11%), IUD in 18 (17.48%), stillbirth in 2 (1.94%) and 72 (69.9%) were admitted to NICU. • Among 47 patients who had no hyperuricemia IUGR was present in 32 (68.08%), 9 (19.14%) had IUD, 1 (2.12%) had stillbirth and 16 (34%) were admitted to NICU. • Hence IUGR and admission to NICU were more significantly more frequent among those with hyperuricemia; p< 0.05. • The mean birth weight of babies was 1.730.48 and 2.020.55 kg among hyperuricemic versus non-hyperuricemic mothers; p= 0.002. • Pregnant women with pregnancy induced hypertension defined as a BP > 140/90 diagnosed at the gestational age > 20 weeks will be recruited through emergency or the outpatient department. • These patients had their uric acid levels measured with an autoanalyzer using a phosphotungstic acid reagent. • All patients underwent antenatal ultrasound with doppler studies in the last trimester to identify IUGR fetuses. • These patients were followed till the time of delivery. • The birth weight, NICU admissions and stillbirths/ intrauterine deaths were documented. • Inclusion Criteria: • Pregnant women after 20 weeks gestational age. • Women with pregnancy induced hypertension as defined above with a BP > 140/90 on two occasions diagnosed > 20 weeks gestational age. • Women of any age and parity. • Exclusion Criteria: • Patients with pre-existing hypertension before 20 weeks of gestation. • A known history of kidney disease identified on history of deranged renal functions. • Women on drugs known to increase uric acid levels like thiazides, aspirin and pyrazinamide. • Patients who did not include their follow up till the time of delivery were not included in the study. CONCLUSIONS • Hyperuricaemia is frequent among patients with pregnancy induced hypertension • Babies of patients with pregnancy induced hypertension with hyperuricaemia had: • significantly higher IUGR • more frequent admissions to NICU • significantly low birth weight. Content goes here… Text… DISCUSSION • Including uric acid in the evaluation of preeclampsia, we can identify a high risk group that is likely to end up in fetal complications. • In the evaluation of gestational hypertension without proteinuria, the absence of hyperuricaemia can identify a low risk GROUP. • Despite the fact that hyperuricaemia is not part of diagnostic criteria for preeclampsia and thus, not typically considered a useful aid to management, several observations have suggested that the presence of hyperuricaemia may identify a form of pregnancy association hypertension with increased risk of preeclampsia. OBJECTIVES • To determine the frequency of hyperuricaemia in patients with pregnancy induced hypertension • To compare the early neonatal outcome between patients with hyperuricaemia and those without hyperuricaemia among patients with pregnancy induced hypertension REFERENCES • Redman CW, Sargent IL. Latest advances in understanding preeclampsia. Science 2005;308:1592-4. • Menzies J, Magee LA, Macnab YC, Ansermino JM, Li J, Douglas MJ, et al. Current CHS and NHBPEP criteria for severe preeclampsia do not uniformly predict adverse maternal or perinatal outcomes. Hypertens Pregnancy 2007;26:447-62. • Zadehmodarres S, Razzaghi MR, Habibi G, Najmi Z, Jam H, Mosaffa N, et al. Random urine protein to creatinine ratio as a diagnostic method of significant proteinuria in pre-eclampsia. Aust N Z J Obstet Gynaecol 2006;46:501-4. • Duley L, Meher S, Abalos E. Management of preeclampsia. BMJ 2006;332:463-8. • Bainbridgea SA, Robertsa JM. Uric Acid as a Pathogenic Factor in Preeclampsia. Placenta 2008;29:67-72. • Powers RW, Catov JM, Bodnar LM, Gallaher MJ, Lain KY, Roberts JM, et al. Evidence of endothelial dysfunction in preeclampsia and risk of adverse pregnancy outcome. Reproductive Sciences 2008;15:374-81. • James MR, Lisa MB, Kristine YL, Carl AH, Nina M, Roberta BN, et al. Uric acid is as important as proteinuria in identifying fetal risk in women with gestational hypertension. Hypertension 2005;46:1263. • Thangaratinam S, Ismail KM, Sharp S, Coomarasamy A, Khan KS. Accuracy of serum uric acid in predicting complications of pre-eclampsia: a systematic review. BJOG 2006;113:369-78.