Download
1 / 37
1.02k likes | 2.56k Vues
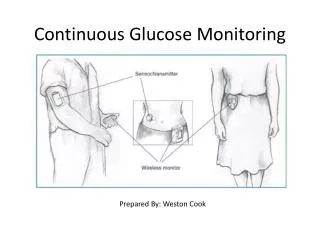
Continuous Glucose Monitoring. Diabetes Management Evolution. Glucose Monitoring. Urine Testing. 1977 Blood Glucose Meter. 2012 Dexcom G4. 2000 First CGM system. 2005-2007 Real-time CGM. Navigator. 2006 Paradigm REAL-Time, combining Insulin Pump and CGM. 1999

E N D
Diabetes Management Evolution Glucose Monitoring Urine Testing 1977 Blood Glucose Meter 2012 Dexcom G4 2000 First CGM system 2005-2007 Real-time CGM Navigator 2006 Paradigm REAL-Time, combining Insulin Pump and CGM 1999 First Animas Pump-R1000 1983 First Minimed Pump-502 1978 First Insulin Pump 1920s Insulin Injections Insulin Delivery NOTE: Only the Medtronic Real-time CGM is approved for use in children and adolescents in the U.S.
Why Continuous Glucose Monitor? • Prevention of hypoglycemia • Prevention of hyperglycemia • Pattern assessment • Basal Testing • Assess the impact of food on blood glucose • Assess the impact of exercise on blood glucose • Behavior modification tool • Alerts/Alarms: Safety, peace of mind…
Hypoglycemia in Children and Adolescents • 657 children followed for 3 years • 8.5% had severe (seizure/coma) hypoglycemia • 27% had moderate (required assistance) hypoglycemia • 75% of seizures occurred at night • Recent CGM data shows seizure may require prolonged severe hypoglycemia prior to event Davis EA, et al. “Hypoglycemia: Incidence and clinical predictors in a large population-based sample of children and adolescents with IDDM” Diabetes Care 1997;20:22-25.
Seizure 17 y.o. Female, A1C 6.2%
14 y.o. male A1C 6.6%, Crews (rowing team) in PM • 5/16/06 5/27/06
Camp Study: Duration of hypoglycemia with and without remote monitoring in 13 y.o. male on MDI No Remote Monitoring <70 mg/dl = 350 minutes <50 mg/dl = 305 minutes “Insulin Rx” is glucagon Remote Monitoring <70 mg/dl = 110 minutes < 50 mg/dl = 10 minutes
Daily Patient Log 400 350 300 250 Glucose (mg/dl) 200 150 Target Range 100 50 0 Breakfast 8:30 am Lunch 12:00 noon Dinner 6:00 p.m. Bedtime 10:30 p.m. Fingerstick Measurement Insulin Bolus
Target Range Daily Patient Log and Sensor Data 400 350 300 250 Glucose (mg/dl) 200 150 100 Fingerstick Measurement 50 Sensor Measurement Insulin Bolus 0 Breakfast 8:30 a.m. Lunch 12:00 noon Dinner 6:00 p.m. Bedtime 10:30 p.m.
What’s the Difference?? CGM adds an additional dimension, the rate of change and direction of change. • 100 mg/dL OR 2. 100 mg/dL dropping at rate of >2 mg/dL/min
Practical Application:Real Life Experience “Paula’s Pearls”
Pearl # 1:Match Device to Patient Needs Size…real estate issues Transmitter Range
Transmitter Range: I can’t find you!!
Pearl # 2 :Match Insertion Approach…Ouch! ◊ Use numbing cream: lidocaine topical Ela-Max cream EMLA cream ◊ Use soap and water to wipe off cream then clean with alcohol
Tape Issues: How do we get this thing to stay on?? IV 3000, Tegaderm, Hy-Tape Coban IV prep- avoid at sensor insertion area “Sandwich”/layer tape Tape Allergies…Ugh!
Pearl # 3: Teach, Teach and Teach Again! Sensor Lag Time Calibration Trend Arrows Glucose Trends/Patterns
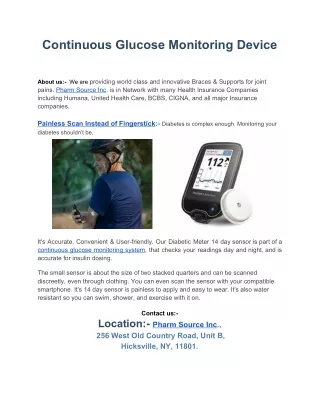
Sensor Lag Time: Why doesn’t the sensor match my fingerstick reading? There is a 10-20 minute lag time between interstitial fluid (ISF) glucose and BG Lag occurs with ALL subcutaneous sensors CGM is a trending device, NOT a treatment device
Sensor Lag Fingerstick Capillary Glucose (SMBG) Interstitial Fluid Glucose (CGM)
QUESTION:When will the ISF glucose and the BG value be the most similar/closest? When BG is stable/not fluctuating rapidly
QUESTION:When using a CGM, when should the patient test their BG with a fingerstick? Before all treatment decisions and insulin To verify symptoms of hypoglycemia Before driving
Calibration: When to calibrate? The accuracy of all the CGM’s are dependent on the calibration phase Devices calibrate in 1-2 hours Must do a fingerstick BG to calibrate Do NOT calibrate when the BG is changing rapidly
Calibration: When is the best time to calibrate? When BG is not changing rapidly
Trend Arrows: Show the direction of change Provides information on the rate-of-change
Activity • Table teams review the CGM downloads • What do you see? • What don’t you see? • Recommendations/Suggestions?
Glucose Trends – CGM Report Post-breakfast excursion
Glucose Trends – CGM Report Post-breakfast excursion Nocturnal lows
Pearl # 4: Respond to Data Change behavior! Pre-bolus Less carbs at breakfast Assess food impact Check basal rates Use alarms
Pearl # 5: Who should wear a CGM? • MOTIVATED patients/parents! • Those willing and able to be educated on the device • Those who are willing to look at and respond to the data! • Those with realistic expectations and who can handle a potentially “rocky” start
Report # 4: Failure to acknowledge alarms and using pump suspend
Report # 5: Pump site failure Pump site failure Insulin via syringe Insulin via syringe