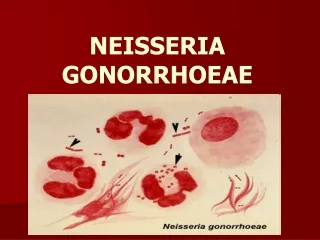
NEISSERIA
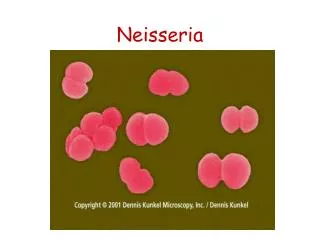
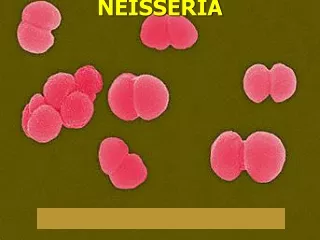
NEISSERIA. Introduction. The Neisseriae are G-ve diplococci Pathogens are:- N.meningitidis N.gonorrhoeae Exacting growth requirements Commensals easy to grow on ordinary media. N. gonorrhoeae. Obligate parasite of human urogenital tract. Morphology: Gram -ve diplococci (bean shaped).

NEISSERIA
E N D
Presentation Transcript
Introduction • The Neisseriae are G-ve diplococci • Pathogens are:- N.meningitidis • N.gonorrhoeae • Exacting growth requirements • Commensals easy to grow on ordinary media
N. gonorrhoeae • Obligate parasite of human urogenital tract. • Morphology: Gram -ve diplococci (bean shaped). • Culture: enriched media (lysed blood or chocolate), moist aerobic atmosphere +5-10% CO2. Temp.35-37oC.
Selective media • Thayer-Martin medium contains vancomycin, colistin, nystatin & trimethoprim. • Colonies: 48hrs incubation.
Identification • Oxidase +ve. • Carbohydrate utilization: N.gonorrhoeae produces acid from glucoseonly. • Slide agglutination with specific antisera (Phadebact test).
Pathogenicity • Causes gonorrhoea • Arthritis, • Septicemia, • Ophthalmia neonatorum.
Gonorrhoea • Acute pyogenic infection of urethra and (in females) cervix. • Acute purulent urethral , vaginal discharge , dysuria • Asymptomatic in females • Rectum & oropharynx may be involved.
Complications • Prostatitis, epididymitis , urethral stricture in males. • Salpingitis , infertility in females • Septicemia • Arthritis • Meningitis (rare).
Diagnosis • Specimen: urethral,cervical smears &swabs (transport medium). • Gram film: intracellular Gram -ve diplococci • Culture: selective media • Oxidase +ve • acid production from glucose • Latex agglutination
Treatment of gonorrhoea • One curative dose • Sens. Testing • Blind treatment: ceftriaxone,ciprofloxacin • Spectinomycin • Penicillin: resistance common.
N. meningitidis • Habitat: human nasopharynx (10-25%) • Similar to N. gonorrhoea but less exacting ? • Can grow in BA, Chocolate agar without selective media from CSF ? • Id. CHO utilization: acid from glucose& maltose.
Antigenic structure • Polysaccharide antigens • Three main groups A,B,C • Other groups Y,W135. • Grouping: slide agglutination with specific antisera
Pathogenicity • Meningococcal meningitis, as a spread from nasopharynx blood stream meninges in susceptible hosts. • Direct spread to meninges • Rash • Adrenal haemorrhage (Waterhouse-Friderchsen syndrome)
Meningitis • Clinically: rapid deterioration of flu like illness • Headache, neck stiffness, +ve kerning’s sign, fever,..… • Diagnosis: CSF + blood culture • CSF: WBC , RBCs • Gram stain: bacteria & cells
Meningitis (Continue) • Culture deposit into blood & chocolate agars and glucose broth 7 cooked meat media • Incubate in air + 5%CO2 • Id : sugar utilization + latex • For partially treated meningitis: detection of bacterial antigen by: latex agglu, CCIE.. for common serogroups of meningitis pathogens.
Treatment • Parenteral antimicrobial • Start blind treatment after collection of specimens by: • Ceftriaxone or cefotaxime • Change later according to sens. Test. • Contacts: rifampicin • Prevention: vaccination (polyvalent)
Commensal Neisseriae • N.pharyngis, N.flava, N.sicca,.. • In mucous mem. Of mouth,nose, pharynx, less common in genital tract. • Differ. From pathogenic one: • grow in ordinary media( no CO2) • at room temp. • rough, pigmented • acid from a number of CHOs
Other causes of meningitis • Bacterial causes: • Three primary pathogens: • N. meningitidis, HI, S.pneumoniae • N.menningitidis all ages • HI 2m-5y • S.pneumoniae all ages but more common in adult with underlying illnesses.
Other causative bacteria (Continue) • E.coli & other coliforms • Listeria • Strept.group B • Salmonella spp. • Favobacteria.. • All common in neonates
Other causative bacteria (Continue • After surgery or trauma • S.aureus • S.pneumoniae • AFB chronic meningitis • Spirochaetes
Other Causes • Viral :enterivirus, Paramyxovirus, Herpes viruses, adenoviruses, arboviruses. • Fungi: yeasts (Candida, cryptococcus spp.) • Aspergillus spp. • Mucor
Findings in CSF Normal CSF: • Clear , colorless • 0-5 lymphocytes • Sterile • 150-450 mg /l protein • 2.8-3.9mmol/l glucose
CSF in bacterial meningitis • Turbid • 500-20,000 cells mainly polys,few lymphocytes • Bacteria in Gram stain • Markedly raised protein • Reduced or absent glucose
CSF in TB meningitis • Clear or slightly turbid • 10-500 cells,mainly lymphocytes( polys early) • AFB in Z-N stain • Grow in LJ medium • Moderately raised protein • Sugar reduced
CSF in viral meningitis • Clear or slightly turbid • 10-500 cells mainly lymphocytes • Stool culture, or serology +ve • Normal or slightly raised protein • Normal glucose
Cerebral abscess • Clear or slightly turbid • Bacteria: S. milleri, Bacteroides, S.aureus. Proteus(Causative bacteria) • 0-500 mainly polymorphs • Often no organisms in CSF • Normal or raised protein • Normal glucose
Complication of meningitis • Death ( 30% with pneumococci,10% Hi & N.meningitidis. • Ventriculitis • hydrocephalus • Paralysis • Cerebral abscess..
Treatment of meningitis • Depends on age ,causal bacteria • Urgent ,parenteral • Ceftriaxone • Neonates: amp+ gm (or ceftriaxone) • Sens.testing • Anti TB