Clinical Plan
This clinical development plan presents the innovative MCC therapy for patients with high-risk non-invasive bladder cancer, particularly for those refractory to BCG treatment. An estimated 60,834 patients are diagnosed annually in the EU and U.S. with a 30% metastatic risk of death within 12 months. With promising phase I/II results showing a complete response (CR) of 46% at the 8 mg dose, our phase III program aims to establish MCC's safety and efficacy as a first-line treatment compared to BCG. Recruitment for the study is set for 12-18 months, targeting a robust 630 patients across multiple centers.

Clinical Plan
E N D
Presentation Transcript
Clinical Plan François Charette, MD Chief Medical Officer
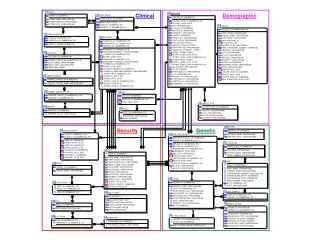
Bladder Cancer Population 60,834 Advanced 30% (Death<12mos. if metastatic ) 202,781 cases annually (EU & U.S. alone) Low (Chemo & TURB) 50% 70,974 Risk Failure to 30% Intermediate 141,947 Superficial 70% 1st line Risk 30% tumor 42,584 12,775 High 20% 8,517 28,389 Risk + 70,973 21,292 Potential MCC patients 21 or 24 doses/patient (chemotherapy costs $500 - $1,000/dose) GLOBOCAN 2002
MCC Clinical Development Plan • Simple rationale • Immunologic mechanism • Chemotherapeutic mechanism • Unmet needs • Issues with efficacy (chemotherapy, BCG) • Issues with safety (chemotherapy, BCG) • Successful Phase I/II studies completed • Majority BCG refractory patients
Phase I-II Results • Safety Results • 9 patients withdrew from the study due to adverse events • (9/130 = 7%). BCG is between 20 and 30%. • Skin rash, possible relationship • Lower abdominal pain/fever/fatigue, related • Pyelonephritis (SAE), possible relationship • Pneumonia (SAE), after one dose of MCC, unknown relationship • Congestive heart failure (SAE), no relationship • Bladder pain, possibly drug related • Bladder pain, possibly drug related • Severe chest congestion, possibly drug related (8 mg) • Bladder pain, possibly drug related (8 mg)
Phase I-II Results 109 patients: 81 received 4 mg, 28 received 8 mg4 mg at 6 months gave a CR of 35%8 mg at 6 months gave a CR of 46%
Percentage of Complete Responders - prior BCG treated patients 50 45 40 35 30 % Complete 4 mg 25 Response 20 8mg 15 10 5 0 12 weeks 24/26 weeks Time post treatment Phase I-II Results 67 patients: 47 received 4 mg, 20 received 8 mg4 mg at 6 months gave a CR of 29.8%8 mg at 6 months gave a CR of 50%
Phase I/II Study Conclusions • In patients with non-invasive bladder cancer, MCC was well tolerated (even in the presence of a disrupted epithelium). • Both studies demonstrated anticancer activity in patients with CIS of the urinary bladder as a second line therapy when patients failed to respond to standard immunotherapy (BCG) and/or chemotherapy, and as first line therapy in some patients • Efficacy was improved with the 8 mg dose compared to the 4 mg dose.
Phase III Program -Growing body of pre-clinical evidence showing the efficacy of MCC -Good Phase II results showing: • Safety • Efficacy -Recognized treatment guidelines -Protocols developed in consultation with FDA -Targeting market access with broad indication -FDA has approved IND
Phase III Program – Part One MCC in BCG refractory non-invasive bladder cancer patients Standard therapy: BCG given the opportunity to succeed in high risk of recurrence/ progression patients • No treatment offering responses over 20% • These patients are truly at high risk • After failure, patients referred for cystectomy
Phase III Program – Part One MCC in BCG refractory non-invasive bladder cancer patients • Recruit in 12-18 months (105 patients) • Endpoint in 12-18 months • Data lock, analysis, report in 6 months • File with registration authorities
Phase III Program – Part Two Randomized, double-blind, multi-centre trial comparing MCC to BCG as first line treatment for patients with non-invasive bladder cancer at high risk of recurrence or progression • Robust: 630 patients, blinded, worldwide • Comparator is the recognized therapy • Safety: superiority • Efficacy: superiority (or non-inferiority)
Phase III Program – Part Two Randomized, double-blind, multi-centre trial comparing MCC to BCG as first line treatment for patients with non-invasive bladder cancer at high risk of recurrence or progression • Recruitment 2 years • Endpoint after 1-2 years for efficacy and safety • Data lock, analysis, report in 6 months • File with registration authorities
Conclusion Population to treat (high risk bladder cancer) 0% 50% 100% 70% respond to BCG 30% refractory Refractory trial 40-60% refractory respond to MCC Comparative trial 82-88% respond to MCC = superiority to BCG