Prehospital Fibrinolysis with Dual Antiplatelet Therapy in Acute STEMI: Clarity Ambulance Substudy
This study investigates the impact of prehospital fibrinolysis combined with dual antiplatelet therapy on acute ST-Elevation Myocardial Infarction (STEMI) patients. It highlights challenges faced in timely fibrinolysis and management of STEMI in ambulances across France, the UK, and Sweden. Results indicate that prehospital management may significantly improve reperfusion rates without increasing bleeding risks. Findings show beneficial effects of using clopidogrel alongside other treatments, underscoring the importance of rapid, effective prehospital care.

Prehospital Fibrinolysis with Dual Antiplatelet Therapy in Acute STEMI: Clarity Ambulance Substudy
E N D
Presentation Transcript
Prehospital Fibrinolysis with Double Antiplatelet Therapy in Acute ST-Elevation Myocardial Infarction: The Clarity Ambulance Substudy
Ambulance Substudy Background • Fibrinolysis for ST-elevation acute myocardial infarction (STEMI) is frequently limited by delays of administration as well as incomplete reperfusion or reocclusion of the infarct-related artery1 • Intensified prehospital management may shorten time to treatment and improve outcomes2 1. Brouwer MA et al. Circulation 2002; 106: 659–665. 2. Morrison LJ et al. JAMA 2000; 283: 2686–2692.
Substudy Sites and Patient Numbers France: 172 patients • L Soulat: 57 • Y Lambert: 48 • F Lapostolle: 28 • F Thieuleux: 21 • C Gully: 10 • D Pollet: 5 • D Galley: 2 • L Olliver: 1 • UK: 40 patients • J Adgey: 27 • J Purvis: 13 • Sweden: 5 patients • J-E Karlsson: 5 217 patients in total
Patient Management: Ambulancevs. Non-Ambulance *p <0.001 versus ambulance patients; values are median unless otherwise specified
0 0.5 1.0 1.5 2.0 2.5 3.0 Angiographic & ECG Parameters: Ambulance vs. Non-Ambulance Event rate (%) Odds ratio (95% CI) Ambulance Non-ambulance p value Ambulance better Non-ambulance better *Complete considered to be >70%; ECG=electrocardiogram
0 0.5 1.0 1.5 2.0 2.5 3.0 Primary Outcome Parameters: Ambulance vs.Non-Ambulance Event rate (%) Odds ratio (95% CI) Ambulance Non-ambulance p value Non-ambulance better Ambulance better *Occluded infarct artery (TFG 0/1) + death + re-MI prior to angiography; NS=not significant
0 0.5 1.0 1.5 2.0 2.5 3.0 Primary Outcome Parameters: Ambulance Subgroup Event rate (%) Odds ratio (95% CI) Clopidogrel Placebo p value Placebo better Clopidogrel better *Occluded infarct artery (TFG 0/1) + death + re-MI prior to angiography
Primary Endpoint of TIMI Flow Grade 0/1, MI or Death Odds ratio (95% CI) 0.60 (0.301.17) Ambulance 0.65 (0.540.77) Non-ambulance Overall 0.64 (0.530.76) 0 0.5 1.0 1.5 2.0 Clopidogrel better Placebo better
Safety: Bleeding Complications TIMI=thrombolysis in myocardial infarction; ICH=intracranial hemorrhage
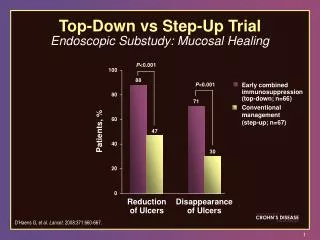
Conclusions • Medical reperfusion of STEMI patients with fibrinolysis, heparin, ASA and clopidogrel is feasible before reaching the hospital in medically equipped ambulances without an apparent increase in bleeding • Early management of patients in the ambulance is associated with shorter ischaemic times and faster reperfusion, with a consistent treatment effect in favour of clopidogrel in comparison with the overall results