Download
1 / 16
160 likes | 286 Vues
Referral Screening and Psychotherapy I ntake of Children in Foster C are. Emily Reich, B.A. University of San Francisco April 29 th , 2012. Background.

E N D
Referral Screening and Psychotherapy Intake of Children in Foster Care Emily Reich, B.A. University of San Francisco April 29th, 2012
Background Multiple mental health problems occur in foster children as a result of the trauma of removal from home, entry into an out of home placement, and frequent placement changes. Long-term, relationship-based psychotherapy significantly reduces many mental health symptoms experienced by these children. Understanding the referrals of these youth for treatment and the mental health profile at the start of treatment is an essential piece of designing and implementing effective mental health interventions.
Hypotheses The existence of mental health symptoms in this population will be fairly high, similar to that of the youth in relevant literature. Due to their background training, therapists will report more emotional problems than referrers. Due to their role in the child or adolescent’s life, referrers will report more behavioral problems than therapists.
Methods: Participants Referrers played a variety of roles in the lives of the referred foster youth. Therapists were generally white, middle aged females who represented a variety of mental health professions.
Methods: Participants The thirty-five referred current and former foster youth were ethnically diverse, usually female, ranging in age from 3.63 years to 29.92 years (M = 14.54, SD = 6.74).
Methods: Participants Referred youth had been removed from home for multiple reasons and experienced an average of 2.41 different placements in the foster care system (SD=2.21).
Methods: Measures A Home Within Screening Form Initial Telephone Questionnaire for Therapists (ITQT)
Example Items from the Screening Form Why now?/Current Problems Is the patient currently violent/suicidal/psychotic? What is the patient’s current psychiatric status?
Example Items from the ITQT • Symptoms at Start of Treatment: (rate each item) • Depression: None Mild Moderate High Extreme • Anxiety: None Mild Moderate High Extreme • Dissociative None Mild Moderate High Extreme Symptoms: • Suicidality: None Mild Moderate High Extreme • Sleep Problems: None Mild Moderate High Extreme • Eating Problems: None Mild Moderate High Extreme • Conduct Problems: None Mild Moderate High Extreme • Enuresis: None Mild Moderate High Extreme
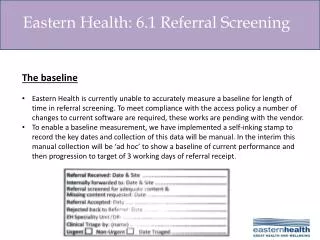
Methods: Procedures Current and former foster youth are referred to therapy. The intake coordinator performs a brief telephone screening. Youth are matched to a local A Home Within therapist. The University of San Francisco’s Foster Care Research Group (FCRG) is notified of the match. A research assistant performs an initial interview with clinicians who agree to participate. A Home Within Referral Forms and FCRG intake interviews for therapists who agree to participate are compared.
Results T-tests were performed to determine the difference of responses between clinicians and referrers.
Results Referred and treated foster youth exhibited a high amount of emotional and behavioral problems, similar to the foster youth studied in previous research. According to both therapists and referrers, most of the foster youth had emotional problems. However, therapists reported these symptoms at a higher rate than referrers. Therapists noted behavioral problems more often in youth than did referrers.
Discussion and Conclusions Therapists report significantly more emotional and behavioral symptoms across a variety of domains, suggesting that the comprehensive assessments of new patients, conducted as treatment begins, allows identification of mental health symptoms beyond those noted by referrers. Accurate clinical assessment of current and former foster youth is important, therefore it is important that these individuals are screened by licensed mental health professionals. It is possible that the specific roles the therapists and referrers have in the lives of the foster youth may have caused the differences in assessments.
Limitations The small size of this population limits the generalizability of this study’s results to the general population of foster youth in treatment. The use of different instruments for referrers and therapists, the screening form and ITQT respectively, may have caused the reports to differ between informants.
Future Directions Researchers have worked with AHW to revise the screening form so that it includes many of the same items of the ITQT, including the symptom checklist. Data collection will continue to increase generalizability to the larger population. The research team will work toward interviewing social workers, foster parents, teachers, and foster youth in the future to compare assessments from more informants.