Download
1 / 59
590 likes | 616 Vues
Learn about the causes of and investigations for haematuria, including definitions, types, systemic and local causes, and laboratory tests.

E N D
Causes of haematuria and Investigations of urinary tract
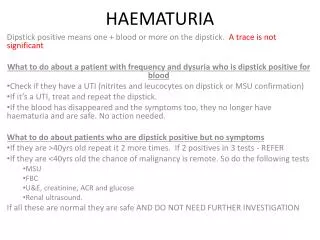
Haematuria • Definition:- presence of blood in urine. • More than 2-3 RBC’s per high power field in a centrifuged specimen is significant.
Microscopic Tiny amount of blood insufficient to stain urine. Detected by dipstick. Macroscopic Substantial hemorrhage into urinary tract. Give urine a brownish or red tinge Haematuria
Depending on timing of haematuria • Initial haematuria: • Usually from prostatic urethra (BPH, prostatic ca) • Total haematuria: • Through out micturation. • From bladder or upper UT. • Terminal haematuria : • At end of micturition. • Signifies severe bladder irritation by stone or infection.
Associated with pain or not. • Painful haematuria: • Associated with inflammation or obstruction. • Upper UT pathologies. • Obstruction due to calculi or blood clots. • Painless haematuria: • In malignancies.
Is there any clot? What is the shape? • Presence of clot- more significant degree of haematuria. • Amorphous clots are from bladder or prostatic urethra. • Vermiform (worm like) clots associated with flank pain- from ureter in upper UT.
Haematuria can be: • True haematuria:- • Due to nephrologic or urologic disease. • Spurious haematuria:- not from urinary system • Due to contamination with menstrual blood. • Fallacious (malingering). • False haematuria:- • High coloured and concentrated urine during hot season. • Due to drugs; rifampicin, pyridium,b complex etc.
Pseudo haematuria can be excluded by urine dipstick and confirmed by microscopy.
Systemic causes • Bleeding disorders. • Blood dyscrasias. • Infective endocarditis.
Drug induced • Cyclophosphomide- hemorrhagic cystitis. • NSAIDS-tubular necrosis. • Antiplatlet drugs- clopidogrel, aspirin. • Anticoagulants- heparin, warfarin. • Analgesic nephropathy- papillary necrosis.
Glomerulo nephritis. Ig A nephropathy. Renal trauma. Renal calculi. Pyelonephritis. Renal cell carcinoma. Transitional cell carcinoma. Cystic d/s of kidney. Hydronephrosis. TB of kidney Renal infraction. Angio myolipoma. Wilms tumor. Congenital malformations- AV malformations (fistulae). Radiation nephritis. Papillary necrosis, a/c pylonephritis in DM Local causes- kidney
Local causes- ureter. • Ureteric stones. • Transitional cell Ca. • Surgical trauma. • Infection .
Local causes- bladder • Transitional cell ca. • Rhabdomyosarcoma. • a/c cystitis. • Bladder calculi. • TB of bladder. • Bilharziasis-parasitic d/s schiztosoma. • Haemangiomas.
Local causes • Bladder neck: • BPH • Carcinoma prostate • urethra • Urethral injuries- RTA etc… • Urethral malignancies. • Stone.
Urine analysis • Clean catch midstream urine is required. • Should be examined while fresh. • Refrigeration lead to sedimentation of phosphates • Storage in a warm environment result in deterioration of formed elements & growth of bacteria.
Physical examination • Colour :normal straw colour. • Black tea colour - haematuria • Changes can also occur in certain diseases, on ingestion of certain foods or medication e.g. pyridium – orange-red, methylene blue – bluish or green colour pink – beets or food dyes, medications like Selenium bluish-grey & brown – a/c porphyria
Odour – aromatic odour mousy odour – infections due to formation of ammonia pungent odour – necrotic bladder tumours or a/c porphyria • Fixed low specific gravity indicates renal tubular dysfunction
Chemical Examination • Dipstick test • quick and inexpensive. • Detecting abnormal substances in urine e.g. blood, protein, glucose etc • Also an indication of pH and specific gravity of urine
Technique • Completely immerse reagent areas on dipstick • Withdraw immediately to prevent dissolution of reagents into the urine • Edge drawn along the rim • Hold horizontally till reading • Compare with the colour chart
Conditions producing false results • Increased level of ascorbic acid conc. • Highly buffered alkaline urine • Out-dated test strips • Any abnormalities found on Dipstick testing should be confirmed by Microscopy.
Light microscopy RBCs, WBCs, Bacteria Protein casts – renal parenchymal d/s. Phase contrast microscopy nature of cells, dysmorphic cells, crystals, bacteria Microscopic Examination
Cytological Examination • For exfoliated cells • Clusters of cells with nucleo-cytoplasmic disparity – characteristic of malignancy • Sensitive and specific for poorly differentiated transitional cell carcinomas of the urinary tract
Bacteriological Culture • Clean-catch, midstream specimen • >100,000/ml – UTI rather than contamination • Urinary tract TB – centrifuged sediment of multiple early-morning specimens cultured on LJ medium • ‘Sterile pyuria’ – pus cells on urine BUT no growth on culture
Renal Function Tests • B. Urea and S. Creatinine – • Elevated levels – indicate significant impairment of renal function • Creatinine clearance – approx. value of GFR (prone to error) • More accurate assessment of GFR – Clearance of Chromium-51 labelled EDTA • Other tests – urinary loss of Na+ - β2-microglobulin - N-Acetyl Glucosamine (tubular enzyme)
Imaging • KUB film (plain abdominal radiograph showing kidneys, ureters and bladder) • The soft tissue shadows of the kidneys, outlined by radiolucent fatty covering, overlie the upper attachments of the psoas muscles. • Ureter – follows the tips of transverse processes of vertebrae, crosses the sacro-iliac joint,heads for the ischial spine before hooking medially towards the bladder base • Full bladder – hazy outline arising from pelvis
Pathologies seen on KUB • scoliosis • metastases • spina bifida • fractures • degenerative d/s of the spine • arthritis • urinary calculi – in region of kidney and along the course of each ureter.
Intra-Venous Urography • Excretory urography / IVP • Mainstay of urologic investigations • Principle – • i.v. contrasts are chemicals to which iodine atoms are attached to absorb X-rays. • Substance filtered from blood by glomeruli and does not undergo tubular reabsorption. • It renders its path radio-opaque.
These agents are potent nephrotoxins and may provoke life-threatening anaphylactic reactions • Used with caution in pts with h/o allergy, atopy and eczema.
Preparation of patient • Laxatives • Modest fluid restriction – avoid dehydration
Technique • contrast media injected through vein in ante-cubital fossa • Observe patient carefully while the first few drops of contrast are injected • 4 films are taken – • 1 minute – Nephrogram renal parenchyma • 3 min –Pyelogram tubules to pelvis and calyces • 20 min –Ureterogram dye in ureter late phase Cystogram • Post-evacuation film lower ureter and residual urine
IVU is valuable to demonstrate • tumours and calculi • Abnormal anatomy • Functional impairment –delayed nephrogram • Space-occupying lesions – distortion of renal outline or failure of part of kidney to function
Nephrotomography • More detailed and accurate visualization of kidneys and pelvi-calyceal system • Several slices of kidney are obtained, beginning posteriorly and advancing anteriorly. • This eliminates overlying gas and faecal matter in the bowel • Lucent areas such as fat and cysts more readily identifiable • Poorly prepared pts can be better evaluated
Retrograde Pyeloureterography • A fine ureteric catheter passed into the ureteric orifice thro’ a cystoscope. • Contrast medium injected into the catheter • Anatomy of the upper urinary tract demonstrated • Possible under topical urethral anaesthesia using a flexible cystoscope
Useful if • there is doubt about intra-luminal lesion or • renal function is deficient • Urine may be collected from kidney for cytologic study, differential renal function • High risk of introduction of infection leading to septicemia
Antegrade Pyelography • Done under local anaesthesia with fluoroscopic or USG guidance • Percutaneous insertion of a small catheter into the pelvicalyceal system done • Contrast medium introduced thro’ the nephrostomy.
Useful when retrograde studies are prevented by obstruction at the extreme lower end of the ureter • Other uses • -adequate drainage of an obstructed pyelonephrosis • -provide access for percutaneous nephrolithotomy
Renal Arteriography • Percutaneous transfemoral renal arteriography. • Uses • evaluation of renal vascular hypertension • therapeutic dilatation of narrow arteries • Applied for d/d of renal masses:-characteristic neovasculature (tumor blush) and pooling of opaque material (puddling) are noted in corkscrew-shaped tumour vessels within the parenchyma -HYPERNEPHROMA
Digital subtraction angiography • Provides visualization of arterial supply of kidneys (on OP basis). • A bolus of contrast material is injected intra arterially. • Computerized subtraction provides a clear view of- • Renal arteries and their branches. • Aorta & • Other abdominal visceral arteries.
Cysto-urethrography • Bladder & urethra evaluated by antrograde or retrograde studies. • useful • In studying dynamics of micturation, evidence of obstruction or reflux of urine. • To demonstrate the extent of urethral stricture, presence of false passages, diverticulae associated with it. • To assess the extent of urethral trauma.
In trauma there is a danger of passage of contrast into circulation. • Lipiodol carries the danger of fat embolus. • Umbradil viscous V is a radio opaque water soluble gel containing lignocaine. • It is injected gently using Knutsson’s apparatus.
Venography • Visualization of IVC by instillation of i.v. contrast percutaneously into femoral vein. • Helpful in evaluating patient with renal cell carcinoma. • Intrinsic involvement and obstruction of IVC and renal veins may be present with carcinoma. • Pre operative evaluation with this study help to determine the surgery.
Ultrasonography • Widely used in urology. • Uses • Size of kidney, thickness of its cortex can be measured. • Presence and degree of hydronephrosis can be found out. • Cystic renal lesion can be distinguished from solid. • provide means of guiding needles into lesion for biopsy or fluid aspiration. • obstructive uropathy can be ruled out. • Trans rectal USG for early detection & staging of prostatic carcinoma. • Biopsies can be obtained as an OP basis.