
LUNG VOLUMES AND DIFFUSION TESTS
E N D
Presentation Transcript
LUNG VOLUMES AND DIFFUSION TESTS Prof. Dr. Deniz DOĞRU ERSÖZ Hacettepe University Faculty of Medicine Pediatric Pulmonary Medicine Unit
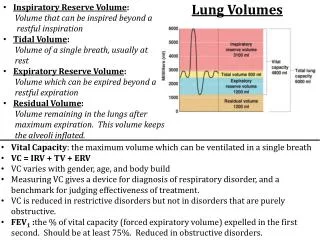
Lung volumes • Functional residual capacity (FRC): The volume of air in the lungs • at the end of atidal breath • Residual volume (RV): The volume of air in the lungs • at the end of a maximum expiration • Total akciğer kapasitesi (TLC): The volume of air in the lungs • at the end of a maximum inspiration
Indications of Lung Volume Measurements • To diagnose restrictive pulmonary disease and assess its severity • To discriminate obstructive and restrictive disease • To diagnose gas trapping • To monitor response to therapy (Bronkodilator, steroid, lung surgery, transplantation, radiation, chemotherapy) • Preoperative evaluation
Measurements of Lung Volumes • FRC is measured generally • TLC is measured by some methods • RV is measured indirectly
Measurements of Lung Volumes • Inert gas dilution: Lung volumes are measured with a known volume and concentration of a gas (Helium) • Nitrogen washout: Lung volumes are measured by expired nitrogen concentration before and after inspiring pure oxygen • Whole body pletismography: Lung volumes are measured by Boyle’s law, with changes in the pressure and volume while breathing in a closed box
Lung volume measurement techniques • Closed circuit, Helium dilution, “multiple breath” • Open circuit, multiple breath N2 washout • Single breath N2 washout • Single breath Helium dilution • Plethysmography • Radiologic methods
Akciğer Hacimlerinin Ölçüm Teknikleri • Closed circuit, Helium dilution, FRC “multiple breath” • Open circuit, FRC multiple breath N2 washout • Single breath N2 washout TLC • Single breath Helium dilution TLC • Plethysmography FRC • Radiologic methods TLC
Closed circuit, Helium dilution, “multiple breath” • The technique relies on inhalation of a known concentration and volume of helium mixture and its homogenous distribution to both lungs
Closed circuit, Helium dilution, “multiple breath” • Helium: preferred as it is not dissolved in blood and can be measured by inexpensive methods • A spirometry is filled with a mixture of helium and oxygen (25-30% oxygen, 10% He)
Closed circuit, Helium dilution, “multiple breath” • Patient is asked to breath quietly (tidal breath) through a sterile mouthpiece with nose clip attached for 30-60 seconds • At the end of a normal tidal breath a valve is opened and the patient commences breathing the helium mixture from the spirometer • Test ends when He is balanced • Test duration 7-10 minutes
Closed circuit, Helium dilution, “multiple breath” • The amount of helium remains constant throughout the test as the circuit is closed • The change in He concentration in the spirometer shows the lung volume of patient
Closed circuit, Helium dilution, “multiple breath” System volume (L) = He added F He initial (% He initial - %He final) FRC = x System volume %He final
Open circuit,multiple breath Nitrogen washout Alveolar nitrogen concentration Nitrogen concentration in the atmosphere 79% = = 79% of the patient’s FRC is nitrogen
Open circuit,multiple breath Nitrogen washout • Measurement of the nitrogen washed out while breathing 100% oxygen • Lung volumes are measured by comparing initial alveolar and exhaled nitrogen concentration • Test duration is generally 3 minutes
Open circuit,multiple breath Nitrogen washout • Patient breaths normally for 30-60 seconds • At the point of a normal end tidal breath the patient commences breathing 100% oxygen • Patient breaths normally for 3 minutes • In this duration, the nitrogen is washed out of the lungs • Expired nitrogen volume is monitorized • Test ends when consecutive 3 expired N2concentration is < 1.5%
Plethysmography • Thoracic gas volume (VTG) is measured • VTG: The gas contained in thorax whether in communication with patent airways or trapped in any compartment of the thorax • VTG: Measured at the end of expiration and equal to FRC • Patient sits in a closed box • The changes in box pressure occur in direct proportion to volume changes occuring in thorax
Plethysmography The test employs Boyle’s law The relationship between the pressure and volume of a gas at a given temperature remains constant (P1xV1 = P2xV2)
Plethysmography Because the relationship of gas/pressure within the lungs and gas/pressure within the box must remain constant, the increase in chest volume is associated with a corresponding change in box pressure
Plethysmography Technique • The patient sits inside the box and the door is closed • While the patient breaths normally, air temperature in the box is allowed to stabilize for 30 seconds • After a period of stabilization, the shutter is transiently closed at the end of a normal tidal expiration
Plethysmography Technique • The patient is asked to pant for several breaths (1-2 breath/second) • Cheeks are supported with hands • Patient should breath with shallow breaths with a constant volume
Panting manuever Properly performed panting manuever Series ofalmost superimposed straight lines separated by only a small thermal drift
Criteria for acceptability • The panting manuever should be at an appropriate volume and rate (1-2 breaths/second) • The loop should be closed and not drift accross the screen • The loop drifting across the screen shows that the thermal equilibrium has not been reached and panting volume is too high • Reported VTG is averaged from 3 to 5 acceptable panting manuevers
Advantages of Plethysmography Measurement of VTG with pletismography is • Easier • Shorter time • More accurate result when compared to dilution methods as it measures whole gas volume in thorax
Disadvantages of Plethysmography • A complex procedure • The manuevers should be instructed carefully in details • Can cause claustrophobia
Interpreting Lung Volumes Factors affecting FRC • Weight, length • Sex • Race • Ethnicity • Changes in body position • Diurnal variations
Increase in FRC • Increase is pathologic • > 120% means air trapping • Emphysema • Asthma • Bronchitis • Lung surgery (Lobectomy)
Increase in RV • Acute asthma attack • Chronic air trapping (Emphysema, obstruction of bronchi) • RV and FRC increase together, generally • As RV increases: More ventilation is done in order to obtain gas exchange VT, respiratory rate increase Work of breathing is increased Hypoxemia, carbondioxide retention
RV/TLC ratio • Describes the percentage of total lung volume that must be ventilated by tidal breathing • 20-35% in healthy adults • RV/TLC : RV veya TLC RV/TLC : TLC Hyperinflation TLC normal Air trapping
Obstructive Diseases • RV is always increased • VC is decreased, TLC remains normal (Air trapping) • VC is normal, TLC is increased (Hyperinflation)
Obstruction TLC TLC TLC FRC FRC FRC RV RV RV RV Normal Air trapping Hyperinflation
Obstructive Diseases • Asthma • Chronic bronchitis • Bronchiectasis • Cystic fibrosis • Emphysema TLC is normal or increased FRC is increased
Restrictive Diseases • FRC, RV, TLC are decreased • Volumes are generally equally reduced • RV/TLC normal
Restriction TLC TLC FRC FRC RV RV Normal Restriction
Restrictive Diseases • Interstitial lung diseases with fibrosis • Pneumonia • Masses in thorax • Chest wall diseases • Pleura diseases • Neuromuscular diseases • Obesity • Congestive heart failure
DIFFUSING CAPACITY • Measures the transfer of oxygen from alveoli to hemoglobin across alveolocapillary membrane • Carbon monoxide is used (CO) • CO, follows the same diffusion way as oxygen asn easy to measure
DIFFUSING CAPACITY • DLCO • Assesses gas exchange of lungs (especially venous oxygenization) • Measures transport carbon monoxide from the alveolacapillary mambrane whose diffusion is limited
Technique • CO, combines with hemoglobin 210 times more readily than oxygen • In presence of normal amounts of Hb and normal ventilatory function, the primary limiting factor to diffusion of CO is the status of alveolocapillary membrane • There is normally little or no CO in pulmonary capillary blood • The pressure gradient causing diffusion is basically the alveolar pressure (PACO) • If the partial pressure of CO in the alveoli and the rate of uptake in gas can be measured, DLCO can be determined