Download
1 / 35
350 likes | 486 Vues
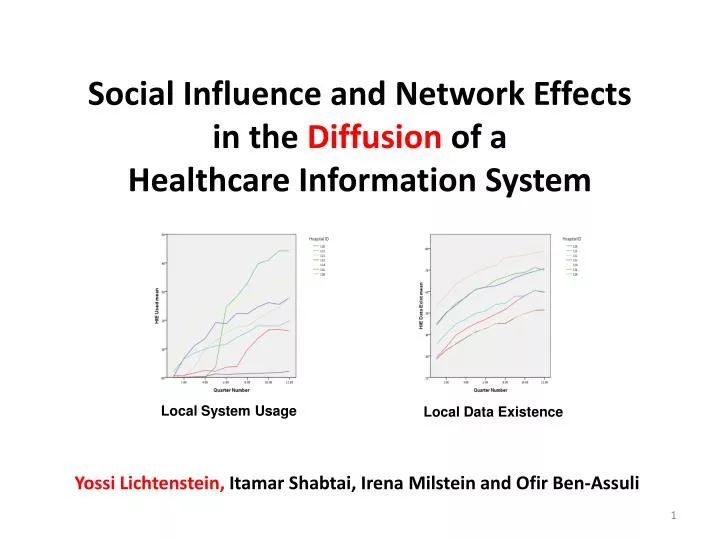
Social Influence and Network Effects in the Diffusion of a Healthcare Information System. Yossi Lichtenstein, Itamar Shabtai, Irena Milstein and Ofir Ben-Assuli. Local System Usage. Local Data Existence. Table of Contents. Part II Model Specification Measures Data per Hospital

E N D
Social Influence and Network Effects in the Diffusion of a Healthcare Information System Yossi Lichtenstein, Itamar Shabtai,Irena Milstein and Ofir Ben-Assuli Local System Usage Local Data Existence
Table of Contents • Part II • Model Specification • Measures • Data per Hospital • Regression • Results • Interpretation • Questions • Part I • Theoretical Background • Empirical context • The System • Diffusion • The Dataset • Questions HIE Diffusion
Part I HIE Diffusion
Theoretical Background • Social Influence • “The main idea of diffusion theory [is] that interpersonal communication with near peers about an innovation drives the diffusion process” (Rogers 2003; p. 342) • Network Effects • “[T]here are many products for which the utility that a user derives from consumption of the good increases with the number of other agents consuming the good” (Katz and Shapiro 1985; p. 424). • Comparison of social influence and network effects • “We found support for both utility and normative explanations” (Kraut et al. 1998) HIE Diffusion
Empirical Context • Clalit* Health Services • 3.8 million customers (half the Israeli population) • 35,000 employees; 9,000 of them physicians • annual budget of about £3 billion • owns 7 general hospitals, 7 other hospitals, including geriatric and paediatric • more than 1,300 community clinics * “General” in Hebrew HIE Diffusion
The System • Health Information Exchange (HIE) • Deployed early 2004 • Retrieves data from other systems at the hospitals and clinics (including historical data) • Provides a comprehensive integrated and real-time virtual-patient-record available at all points of care HIE Diffusion
Diffusion • The connection of other systems to the HIE system was gradual, done both by a central unit of five technicians and by distributed hospital teams, totalling about thirty technicians • We focus on the choice facing a physician at A&E, either to observe the patient’s historical data on the HIE system or not to observe it HIE Diffusion
The Dataset • All patient visits (Referrals) to all A&E departments from January 2004 to Decermber 2007 • Referrals – about 2.25 million • patient data & physician identification • indication if detailed patient data existed • idication if the system was used by the physician • Physicians (n=3,261) • autonomous to use/not-use the system • active for 6 quarters, on average • Active physicians (n=274) • practiced at least 6 quarters and had at least 1,000 referrals • these 8.4% of physicians are responsible for 32.4% of all referrals HIE Diffusion
Questions • How to increase system usage? • Does existence of data influence diffusion? • How does usage rate evolve? • Other perspectives? HIE Diffusion
Part II HIE Diffusion
Model Specification Y(i, j, t) = a Local System Usage(i, t-1) + b Local Data Existence(i, t-1) + c Patient Attributes(i, t) + d Physician Attributes(j, t) + ε(i, j, t) • Y(i, j, t)=1 if physician i observes patient j’s historical data at time t; 0 otherwise • Local System Usage(i, t-1)is the fraction of referrals where the system has been used at the physician i’s hospital in the previous time period • Local Data Existence(i, t-1)is the fraction of referrals at the physician i’s hospital in the previous time period where historical data about patients exist (not necessarily patient j) • Patient Attributes(j, t) are observable characteristics of patient j at time t • Physician Attributes(i, t) are observable characteristics of physician i at time t • ε(i, j, t)is an error term Following Goolsbee and Klenow (2002) who studied the diffusion of PCs in the US HIE Diffusion
Data per Hospital Local System Usage Local Data Existence HIE Diffusion
Regression • Mixed linear regression (McCulloch and Searle 2000) • Physician = subject • Quarter = the repeat unit • The covariance structure is a first-order autoregressive structure with homogenous variances (AR1): the correlation between any two quarters is equal to ρfor adjacent quarters, ρ2 for quarters that are separated by a third, and so on HIE Diffusion
← Results
Interpretation • On average, an additional 1% in average usage at the (active) physician’s hospital in the previous quarter, increases usage by 0.5% • On average, an increase of 1% in data existence at the hospital level, increases HIE usage by 0.05%.This is about a tenth of the usage (social) influence coefficient • (for an internal medicine subset, numbers are 1% and 0.1%) HIE Diffusion
Questions • How is this case related to Decentralization and Flexibility? • All the organizations that have shown the effectiveness of a multifunctional electronic health records developed these systems locally, over years and with clinical champions (Goldzweig et al. 2009). • Does this study quantify locality, gradual deployment and peer influence? HIE Diffusion
Backup Slides HIE Diffusion
Theoretical Background HIE Diffusion
Social Influence • “[Diffusion of innovation is] the process by which an innovation is communicated through certain channels over time among the members of a social system” (Rogers 2003; p. 11) • “The main idea of diffusion theory [is] that interpersonal communication with near peers about an innovation drives the diffusion process” (Rogers 2003; p. 342) • Social learning (Bandura 1977) posits that individuals learn from observing other people’s activities, and that both verbal communication and non-verbal behaviour are important in behaviour change HIE Diffusion
Network Effects • “[T]here are many products for which the utility that a user derives from consumption of the good increases with the number of other agents consuming the good” (Katz and Shapiro 1985; p. 424). • The three main sources: • Direct physical effect, as with litteral-networks such as telephones • Indirect effect, such as in computers where the amount and variety of software for a given computer is dependent on of the number of computers that have been sold (complementary goods) • Whenthe quality and availability of post-purchase service depend on the experience and size of the service network which vary with the number of units sold. • More subtle sources include product information that is more easily avaialble for popular brands, market share as a signal of quality and ”purely psychological, band-wagon effects” (Katz and Shapiro 1985; footnote, p. 424). HIE Diffusion
Integration of Social Influence and Network Effects Kraut, Rice, Cool, Fish, Varieties of Social Influence: The Role of Utility and Norms in the Success of a New Communication Medium*, Organization Science, 9(4), 1998 • “Some commentators have attempted to pit utility theories and normative theories ... against each other. They argue that the objective utility of technology is far less important ... than are the relatively arbitrary views ... that social groups impose upon it” • “In contrast, we attempt to show ... that the two models are complementary, compatible, and reinforcing” *video telephony HIE Diffusion
“We found support for both utility and normative explanations” (Kraut et al. 1998) • Utility • People who used one video telephony system tended to use the other system as well • People in the most communication-intensive jobs were the most likely to use video telephony • People with less analyzable jobs used more video • Normative • People used a particular system more when • more people (in general) were using it • more people in their ownwork groups were using it • The effects of social influence in the work group were strongest among the people most integrated with the group HIE Diffusion
Application HIE Diffusion
Social Influence • The local usage rate represents the observed behaviour of peers at the physician’s locality • We expect that a physician learns from her peers, namely that HIE usage is a result of social learning (Bandura 1977, Rogers 2003, Fichman 2004) • Specifically, a physician at a hospital where the usage rate of the HIE system was high at the previous time period, would mimic her peers and would be more likely to use the system • Similarly, for ERs where usage rate is low, there would be less social learning of a new behaviour and the physician would be less likely to use the system HIE Diffusion
(Indirect) Network Effects • Local rate of data existence during the previous period represents indirect netweork effects (Katz and Shapiro 1985) or a complementary-goods effect (Goolsbee and Klenow 2002) • Namely, the data is complemntary to the system: • when detailed patient data are not available, the demographic data about the patient is of small value • when the HIE system contains data about lab results, imaging results, etc. it is much more valuable • A physician at a hospital where data on patients were readily available (because local surgeries were connected to the system), would be inclined to use the system; similarly, if local experience that the system includes little data, the value of the system is perceived to be limited, and a physician would be less likely to use the system HIE Diffusion
Discussion HIE Diffusion
Summary of Results • Support for the existence of both social influence and complementary-goods network effects in HIE diffusion • Social influence is much stronger – ten times stronger – than network effects • We interpret this as a consequence of the strong organizational and professional structures and culture in healthcare and in the HMO • The nature of the data – an electronic patient record – may also explain the result, because these records are not yet considered critical for ER practices HIE Diffusion
Contributions & Limitations • Explicitly describing, measuring and comparing the effect of social influence and indirect network effects • Observations about the diffusion of healthcare IT that could help other organizations involved in similar efforts • Most effort should be invested in social and organizational influence; investment in populating data in systems and networks should remain secondary • Difficult to generalize from the specific healthcare context • Not yet fully developed analysis HIE Diffusion
Further Research • Complete the analysis • Other opportunities with this dataset • Tie diffusion to subjective value of information (TAM) • Detailed analysis of ‘organizational shocks’: early months at the Early Adopter, second, take-off, year at the ‘Rational Hospital’ • Comparison between early adopters and laggards – are there other characteristics of the diffusion process between them? • Identification of Champions (physicians with high or fast increasing rate of usage) and their influence on their units • Do patients influence diffusion? For example, 200 patients were treated 50 or more times in our dataset HIE Diffusion
Thank you! HIE Diffusion
More Tables HIE Diffusion
← Results
← Referrals HIE Diffusion
← Active Physicians HIE Diffusion