Download
1 / 57
730 likes | 1.41k Vues
Pelvic Inflammatory Disease. DR. EBTIHAG HASHIM CONSULTANT OBS & GYNE MINIMAL ACCESS ENDOPELVIC SURGERY. Pelvic Inflammatory Disease (PID). Infection of the upper female genital tract. Refers to the clinical syndrome among women resulting from infection.

E N D
Pelvic Inflammatory Disease DR. EBTIHAG HASHIM CONSULTANT OBS & GYNE MINIMAL ACCESS ENDOPELVIC SURGERY
Pelvic Inflammatory Disease (PID) Infection of the upper female genital tract. Refers to the clinical syndrome among women resulting from infection. Includes endometritis (infection of the uterine cavity). Salpingitis (infection of the fallopian tubes) MucopurulentCervicitis (infection of the cervix). Oophoritis (infection of the ovaries).
Pathologic Processes of PID • PID has a broad clinical spectrum that includes • acute PID • B. silent PID • C. chronic PID • D. postpartum/postabortal PID
Relevance to Women’s Health: • Commonly occurs in women <35 years. • Rarely occurs before menarche, after menopause or during pregnancy. • About 1.2 million women are treated for PID. • Over 100,000 women with PID are hospitalized each year. • About 15% are acutely ill that require intensive inpatient treatment. • Approximately 85,000 women with mild or moderate PID who currently are being hospitalized, treating them as outpatients may save around $500 million each year.
Causative Agents of PID • NeiserriaGonorrhoeae and Chlamydia trachomatis are the 2 major causative organisms. • Chlamydia trachomatis is the predominant STD organism causing PID. • In the U.S., the role of NeisseriaGonorrhoeae as the primary cause of PID has decreased. • Other agents: Mixed infection caused by both aerobic and anaerobic organisms • Recent studies demonstrate the presence of Bacterial Vaginosis and trichomoniasis in cases of confirmed PID
Causative Agents of PID • Cytomegalovirus (CMV) has been found in the upper genital tracts of women with PID. • Enteric gram-negative organisms (E-coli) • Peptococcus species • Streptococcus agalactiae • Bacteroidesfragilis • Mycoplasmahominis • Gardnerellavaginalis • Haemophilusinfluenzae
Signs & Symptoms of PID • The patient presents with lower abdominal pain, fever, vaginal discharge, and/or abnormal uterine bleeding. • Symptoms frequently occur during or after menses. • Peritoneal irritation produces marked abdominal pain with or without rebound tenderness. • The abdomen should be palpated gently to prevent abscess rupture.
Relevance to Women’s Health • Is one of the major causes of gynecologic morbidity. • Infertility. • Ectopic pregnancy • Chronic pelvic pain • Diagnosis and treatment must be prompt to avoid these conditions.
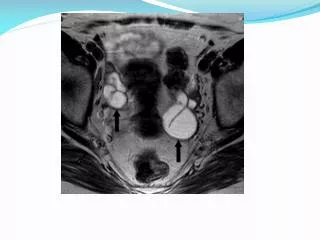
ChlamydialPyosalpinx • Pelvic inflammatory disease, proven ChlamydialPyosalpinx. • Right tube is swollen and tortuous (arrow)
Cervicitis • The cervix appears red and bleeds easily when touched with a spatula or cotton swab. • Mucopurulent discharge is yellow-green. • Contains >10 polymorphonuclear WBCs per oil immersion field (using Gram stain).
Acute Salpingitis • Onset is usually shortly after menses. • Lower abdominal pain becomes progressively more severe, with guarding, rebound tenderness, and cervical motion tenderness. • Involvement is usually bilateral. • Nausea and vomiting occur with severe infection. • In the early stages, acute abdominal signs are often absent
Acute Salpingitis (PID) • Bowel sounds are present unless peritonitis with ileus has developed. • Fever, leukocytosis, and mucopurulent cervical discharge are common • Irregular bleeding and bacterial vaginosis often accompany the pelvic infection.
Complications of PID • Tubo-ovarian abscess develops in about 15% of women with salpingitis. • It can accompany acute or chronic infection • The tube and ovary can become completely matted together. • May require prolonged hospitalization, sometimes with surgical percutaneous drainage. • Rupture of the abscess is a surgical emergency • Rapidly progressing from severe lower abdominal pain to N & V, generalized peritonitis, and septic shock
Tubo-ovarian abscess • Pyosalpinx, in which one or both fallopian tubes are filled with pus, may also be present. • Hydrosalpinx (fimbrial obstruction and tubal distention with nonpurulent fluid) develops if treatment is late or incomplete. • The consequent mucosal destruction leads to infertility. • Hydrosalpinx is generally asymptomatic but can cause pelvic pressure, chronic pelvic pain, or dyspareunia. • Women with HIV infection are more likely to have tubo-ovarian abscess
Tubo-ovarian abscess • Here at least the ovaries, tubes and uterus can still be recognized as separate structures
Fitz-Hugh-Curtis syndrome • Can be a complication of gonococcal or chlamydialsalpingitis. • Characterized by right upper quadrant pain in association with acute salpingitis, indicating perihepatitis. • Acute cholecystitis may be suspected, but signs and symptoms of PID are present or develop rapidly.
Diagnostic Studies: • CBC with differential • Erythrocyte Sedimentation Rate • Cervical cultures • Blood Cultures • Urine Pregnancy Test • Rapid Plasma Reagin (RPR) • Cervical infection due to N. Gonorrhoeae can also be diagnosed by Gram stain showing intracellular gram-negative diplococci
Diagnostic studies • Leukocytosis is typical. • Pelvic ultrasonography may be used when a patient cannot be adequately examined because of tenderness or pain. • When a pelvic mass may be present, or when no response to antibiotic therapy occurs within 48 to 72 h. • Laparoscopy should be performed only if the diagnosis is uncertain or if the patient does not promptly improve with medical therapy.
CDC’s Minimum Criteria for Empiric Treatment of PID • Lower Abdominal Tenderness. • Adnexal Tenderness. • Cervical Motion Tenderness.
Diagnosis • And one or more minor criteria • Temperature over 100.9F or 38.3 C • White Blood Cell count > 10,000 • Elevated ESR • Elevated C-reactive protein • Pus in cul-de-sac • Pelvic abscess or inflammatory complex • Cervical Mucus findings • Gram Stain: Gram Positive diplococci • Intracellular parasites
Diagnosis • ESR and C-reactive protein are elevated in many disorders and are therefore not specific for PID. • All three major criteria and at least one minor criterion must be present to diagnose PID.
TreatmentGoals & Benefits • Therapeutic goals include complete resolution of the infection and prevention of infertility and ectopic pregnancy.
Management Outpatient • Regimen A: • Initial Treatment at Diagnosis • Ofloxacin 400 mg orally BID for 14 days (95% cure) Or • Levofloxacin 500 mg orally once daily for 14 days With or without: • Metronidazole 500 mg orally twice a day for 14 days.
Management Outpatient: Regimen B • Ceftriaxone 500 mg IM in a single dose Or • Cefoxitin 2 g IM in a single dose and Probenecid, 1 g orally administered concurrently in a single dose Or • Other parenteral third-generation cephalosporin (ceftizoxime or cefotaxime) Plus • Doxycycline 100 mg PO BID for 14 days (75% cure) With or without • Metronidazole 500 mg PO BID for 14 days
Management Inpatient • Toxic appearance • Unable to take oral fluids • Unclear DX • Appendicitis • Ectopic Pregnancy • Ovarian torsion • Pelvic abscess • Pregnancy • HIV positive • Outpatient TX failure
Inpatient Treatment Regimens: • General: Treat for at least 48 hours IV • Regimen A • Cefotetan 2g IV q12 hours OR • Cefoxitin 2g IV q6 hours Plus • Doxycycline 100 mg orally or IV every 12 hours
Inpatient Treatment • Regimen B • Clindamycin 900 mg IV q8 hours Plus • Gentamicin 2 mg/kg IV loading dose, then 1.5 mg/kg IV q8h • Discharge Regimen (after IV antibiotics) • Doxycycline 100mg PO BID for 10 days or • Clindamycin 450mg PO QID for 14 days
Alternative Parenteral Regimens • Ofloxacin400 mg IV q 12 hours Or • Levofloxacin500 mg IV once daily With or without • Metronidazole500 mg IV every 8 hours Or • Ampicillin/Sulbactam 3 g IV every 6 hours Plus • Doxycycline 100 mg orally or IV every 12 hours
Prognosis • Therapy using antibiotics alone is successful in 33-75% of cases. • If surgical therapy is warranted, the current trend in therapy is conservation of reproductive potential with simple drainage and copious irrigation or unilateral adnexectomy, if possible. • Further surgical therapy is needed in 15-20% of cases so managed.
Prognosis • Chronic pelvic pain occurs in approximately 25% of patients with a history of PID. • This pain is thought to be related to cyclic menstrual changes, but it also may be the result of adhesions or Hydrosalpinx. • Impaired fertility is a major concern in women with a history of PID. • The rate of infertility increases with the number of episodes of infection. • The risk of ectopic pregnancy is increased in women with a history of PID. • Ectopic pregnancy is a direct result of damage to the fallopian tube.
Prevention • Randomized controlled trials suggest that preventing chlamydial infection reduces the incidence of PID. • Other methods of preventing PID and STD include reducing the number of sexual partners, avoiding unsafe sexual practices, and using condoms with spermicide. • Use of mechanical barriers with spermicide also decreases the risk of acquiring STDs. • Notification of the female sex partners of men infected with Chlamydia trachomatis is recommended
Surveillance • At all levels, PID surveillance is affected by four main constraints: • PID is difficult to diagnose accurately. • PID is diagnosed in a wide variety of clinical settings. • Microbiology test results are needed to determine the etiology of PID.
Patient Education • When medical-care messages are clear, explicit, relevant, and rigorously delivered by providers, patients are likely to comply. • Reinforcement of these messages can be achieved by providing written information. • Information on written materials for patient distribution can be obtained from CDC or local and state health departments
Controversies Surrounding PID • The exact incidence of PID is unknown • The disease cannot be diagnosed reliably from clinical signs and symptoms. • Laparoscopy exam of the pelvic organs continues to be the "gold standard" approach to diagnosis of PID. • But, because this is a surgical procedure which requires an incision in the abdomen, the high priority is to design and development of non-invasive techniques, with smaller costs and fewer risks. • OC may reduce the risk of PID that is not attributable to C. trachomatis.
ANY QUESTIONS ?????
Questions 1: Pelvic inflammatory disease (PID) in women is most commonly caused by: A. Leptotrichiabuccalis B. Treponemapallidum C. Chlamydia trachomatis D. Bacillus anthracis E. Boreliaburgdorferi
Answer The correct answer is #C. Chlamydia Trachomatis
Question 2: IUD use has been linked with: A. pelvic inflammatory disease B. tubal infections C. uterine infections D. all of the above E. none of the above
Answer The correct answer is #D. All of the above
Question 3: Which of the following conditions is not a risk factor for pelvic inflammatory disease (PID)? A. Smoking B. Multiple sexual partners C. Young age at first intercourse D. Hepatitis B E. Intrauterine device (IUD)insertion
Answer • The correct answer is D: Hepatitis B is not a known risk factor for PID.
Question 4: Which of the following is not used to treat symptoms associated with pelvic inflammatory disease (PID)? A: Nitrofurantoin B: Ceftriaxone C: Ampicillin D: Ofloxacin E: Cefoxitin
Answer • The correct answer is A: • No data suggest that Nitrofurantoin is an appropriate oral regimen for the tx of PID. • Most patients are now managed as outpatients. • One outpatient regimen is Cefoxitin and probenecid taken orally in a single dose. • Alternatively, ceftriaxone (less active against anaerobic bacteria compared to Cefoxitin) can be taken once IM with doxycycline orally twice daily for 14 days. • Another regimen is ofloxacin taken orally for 14 days with either clindamycin or metronidazole, which also are taken orally for 14 days.
Question 5: (T/F): The major criteria for the diagnosis of pelvic inflammatory disease (PID) include • Leukocytosis • elevated C-reactive protein (CRP) • elevated erythrocyte sedimentation rate (ESR) • fever.