Chapter 19: Higher mental functions
Chapter 19: Higher mental functions. Chris Rorden University of South Carolina Norman J. Arnold School of Public Health Department of Communication Sciences and Disorders University of South Carolina. Methods of Study. How do we infer brain function?

Chapter 19: Higher mental functions
E N D
Presentation Transcript
Chapter 19: Higher mental functions • Chris Rorden University of South Carolina Norman J. Arnold School of Public Health Department of Communication Sciences and Disorders University of South Carolina
Methods of Study • How do we infer brain function? • Classically, we examined what went wrong when someone had a disorder within the brain and inferred that their injury was crucial for this task. • Example: Patients with left frontal cortex injury have non-fluent speech. • Now we visualize brain structures and localize functional areas using advanced equipment and technology • Example: The left frontal cortex is activated during speech production.
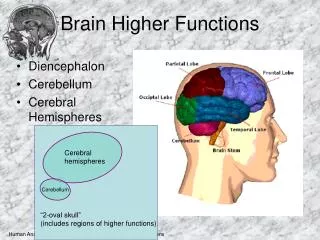
Functional Localization (previous lectures) • Frontal Lobe • Executive function • Planning • Sequencing • Initiation – inhibition • Voluntary movements • Working memory • Occipital Lobe • Vision (Field cuts) • Temporal Lobe • Encoding long-term memories • Language comprehension • Hearing • Parietal Lobe • Reading/Writing • Praxis • Spatial processing (neglect)
Functional Localization • Functionalization occurs over period of time. Brain becomes more specialized with development • People who suffer brain injury early in life will utilize existing brain regions in novel ways. • Plasticity allows compensation
Cerebral Dominance & Functional Specialization • Brain preprogrammed for different uses of right and left hemispheres • Left Hemisphere • Most people have left hemisphere dominant for language • Left hemisphere is called “Dominant” hemisphere • Right handed people have longer planum temporale in left hemisphere which may be biased for use by dominant hemisphere
Right hemisphere functions • Right hemisphere involved in visual-spatial and constructional tasks, emotion and emotional intonation of speech and music. • Right hemisphere is often referred to as the “Minor” Hemisphere • Patients with injury to right cortex often exhibit neglect. • Studies of lateralization can include tests such as Wada test – Today most studies use fMRI for this purpose
Speech and Language Disorders • Motor Speech Disorders • Dysarthria - Paralysis or Paresis of Muscles • Flaccid – LMN problem – hypernasal, breathy speech and imprecisely articulated consonants • Spastic – UMN – Harsh, strained / strangled speech with slow articulation • Hypokinetic – Basal ganglia – variable rate, excessive variation in loudness and timing with distorted vowels • Mixed – Combination of other dysarthrias • Apraxia of speech - No Paresis, Programming Disorder
Language Disorders • Aphasia • Broca’s Aphasia - Broca’s Area • Wernicke’s Aphasia - Wernicke’s Area • Global Aphasia - Wide area • Conduction Aphasia - Angular gyrus or inf. PL • Anomic Aphasia - Angular Gyrus • Transcortical Aphasia • Subcortical Aphasia
Language Production • Broca’s Area (1861) • Difficulty in speech production • Loss of ability to repeat speech • Comprehension intact • Foot of 3rd frontal convolution (BA 44) • Left hemisphere (1865) • Except left handers
Language Comprehension • Wernicke’s Area (1874) • Normal production (speech sounds and fluent nonsense) • Sounds okay if you do not know the patient’s language (e.g. Chinese Wernicke’s aphasic would sound fine to me) • Unaware of deficit • Impaired comprehension • Left hemisphere • Superior temporal gyrus(BA 42, 22)
Wernicke’s prediction • Predicted two language centers: • Broca’s Area: speech articulation. • Wernicke’s Area: language comprehension. • Predicted 3rd Syndrome: • Disconnection syndrome • ‘Conduction aphasia’ • Damage to arcuate fasciculus
Conduction aphasia • Can comprehend speech • Difficulty in repeating speech • phonemic paraphasias (substitution errors) • Lesions in Temporal Parietal Junction that knock out underlying white matter • Patients with damage ONLY to the arcuate fasciculus can still generate speech. • Why? Other pathways
Wernicke-Lichtheim (1885) Schema • From auditory input (a) to motoric articulation of speech (m) Concepts(Distributed) Broca’s Aphasia Wernicke’s Aphasia Conduction aphasia
4: Transcortical Motor Aphasia • Disconnection of Broca’s from concepts • Speech is slow, terse • Can comprehend speech • Found after damage to the frontal lobes • Unlike Broca’s Aphasics, can repeat phrases when spoken to • direct Wernicke’s to Broca’s pathway intact
6: Transcortical Sensory Aphasia • Disconnection of Wernicke’s from concepts • Can repeat words • Speech is articulate nonsense • Unable to comprehend speech • Found after damage to the posterior language area
7 Pure Word Deafness • Loss of ability to understand spoken speech. • Normal speech, reading, writing • Behaviour and anatomy dissociate from Wernicke’s aphasia • Written comprehension intact, intact written/verbal production.
Language Disorders • Alexia • with agraphia - supramarginal or angular gyrus • without agraphia - medial occipital and temporal L. • Aphasic alexia • Deep dyslexia – large mixed lesions • Surface dyslexia – Anterior left hemisphere • Agraphia • Pure agraphia - left superior frontal or parietal regions • Phonological agraphia • Lexical agraphia
Alexia without agraphia • Disconnection of angular gyrus from visual inputs • Language outputs intact • Patients cannot read • Writing preserved • Rare: left and right pathways to angular gyrus • Requires damage to • posterior callosum • left occipital lobe • Without damage to left angular gyrus
Apraxias • Apraxias (Other than Speech) • Difficulty in carrying out learned voluntary motor acts • Constructional: visual-spatial difficulty from RH • Dressing: Spatial perception of clothing in relationship to body • Oculomotor: Difficulty in gaze • Gait: Problems in walking • Ideomotor: Trouble following commands • Ideational: Trouble with multistep tasks – trouble with use of objects – may confuse objects use • Limb-Kinetic: Trouble with one limb only
Anatomy of aphasia Conduction Transcortical- motor Anomic Broca’s Global Wernicke’s Transcortical- sensory