Criteria for Judging Abnormality
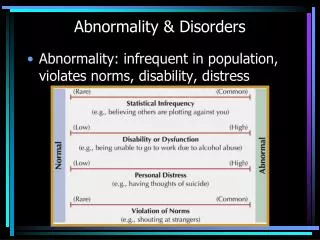
Criteria for Judging Abnormality. How do we decide what qualifies as a mental disorder that needs medical treatment? Statistical infrequency Norm violation Personal suffering. Criteria for Judging Disorders. Statistical frequency

Criteria for Judging Abnormality
E N D
Presentation Transcript
Criteria for Judging Abnormality How do we decide what qualifies as a mentaldisorder that needs medical treatment? • Statistical infrequency • Norm violation • Personal suffering
Criteria for Judging Disorders • Statistical frequency Common or rare? If it applies to most people, it can’t be abnormal • Norm violation Is it outside of culturally accepted or “normal” behaviors? APA is moving away from this in modern multi-cultural society
Criteria for Judging Disorders • Personal suffering • Is it causing harm or distress to self or others. Is it interfering with life? • Is it maladaptive? • This is the most important criteria
When considering whether something is abnormal, Psychologist do NOT consider: race, gender, income. Although critics point out that many “norms” are still defined by a white male perspective.
DSM-IV Classification System The DSM is the Diagnostic Statistical Manual of Mental Disorders. It is the “Psychiatrist’s Bible” Therapists can look up symptoms and conditions to find the proper diagnosis
DSM-IV Classification System • Person is evaluated on 5 dimensions, or axes • Axis I: Diagnosed mental disorder • Axis II: Personality disorders or mental retardation • Axis III: Medical conditions relevant to person’s mental or behavioral problems • Axis IV: Experienced difficulties important for understanding social, environmental, and cultural context in which psychological problems appear • Axis V: Rating (from 1 to 100) of current level of psychological, social, and occupational functioning
DSM-IV Classification System Main Idea: • Therapist looks at whole person and all aspects of situation before making diagnosis
Advantages and Disadvantages of Diagnostic Labels Advantages: Doctors, patients and insurance use the same criteria and use standardized terminology. Disadvantages: Once you label someone it can become a self-fulfilling prophecy. (Rosenhan Study) Some patients feel stigma of label
Anxiety Disorders Person experiences anxiety (mental stress, worry) that is so intense and long-lasting that it disrupts a person’s daily functioning
Anxiety Disorders Phobia: An intense, irrational fear of an object or situation that is not likely to be dangerous • Person usually realizes that fear makes no sense • Agoraphobia – fear of public spaces • Social phobia – fear of interacting with people or public speaking or performance
Phobias are often treated with SystamaticDesensetization Having the patient become less sensitive to the phobia, by using a system of mental relaxation exercises while visualizing or imagining the source of the phobia. -create an anxiety hierarchy
Anxiety Disorders Post-Traumatic Stress Disorder (PTSD): After stressful or traumatic event, person experiences anxiety, nervousness and may mentally “re-live” the trauma • War Vets, Disaster survivors, Rape victims
Anxiety Disorders Obsessive-Compulsive Disorder (OCD): Person is bothered by persistent, recurring, upsetting, and unwarranted thoughts (obsessions) that motivate repetitivebehaviors(compulsions) The compulsion (behavior) eases the obsession (thought or anxiety)
Other Anxiety Disorders Panic disorder – sudden, unpredictable, overwhelming worry. Hyperventilating, need to “escape” Generalized Anxiety disorder – near constant worry about lots of things in general, but nothing in particular. An extreme worrywart. Example: Piglet
Somatoform Disorders Person shows symptoms of a somatic, or bodily, disorder even though there is no physical cause. It is biologically unfounded, but that doesn’t mean they are “faking” or not really feeling it. It’s all in their mind = Somatoform
Somatization Disorder – pain or stomach ache, itching, etc. for no physiological reason • Conversion Disorder – patient converts psychological distress into specific motor or sensory disorder. -- can’t move legs, but muscles are fine • Hypochondriasis – Belief that one has a severe illness or disease -- cough once and rush to the doctor convinced you have pneumonia
Mood Disorders Conditions in which a person experiences extreme moods, such as depression or mania, especially when the moods are not consistent with surrounding events • If you get sad when a family member dies, you do NOT have depression
Major Depressive Disorder: Ageneral lack of interest in the world. Persistent sadness. Lack of energy. Loss of appetite or overeating for comfort. Suicidal thoughts. Treatment - the neurotransmitter serotonin regulates mood, so antidepressant drugs block the reuptake of serotonin so more of it stays in the blood. Selective Serotonin Reuptake Inhibitors (SSRIs) Paxil, Zoloft
Cognitive therapy (talk therapy) can also be successful. Help the patient understand or think through why they are depressed and what they should do about it. How do their beliefs or interpretations make them depressed? • For extreme depression, electroconvulsive (shock) therapy sometimes works.
Mood Disorders Bipolar Disorder: Extreme Mood Swings. A person alternates between deep depression and mania • Mania is a very agitated, usually elated, emotional state • Treated with anti-depressants and lithium carbonate • Previously called Manic-Depressive.
Mood Disorders Seasonal Affective Disorder (SAD): not normally depressed, but seasonal change (mostly to fall or winter) throws you into depression. -- treated with light therapy
Personality Disorders Personality disorders are long-standing, inflexible ways of behavior that are dysfunctional styles of living Can use MMPI test to diagnose. • Narcissistic personality: self-centered, constant bragging, putting down others, needs attention.
Borderline personality: Impulsive, highly emotional, reckless, constant drama, unstable. • Dependent personality: Depends on others, no confidence, won’t make decisions, fixate on a caretaker • Oppositional Defiant Disorder Defiant, will not accept any authority, disagrees for the sake of disagreeing, angry outbursts.
Antisocial Personality • Impulsive, often criminal, behavior that harms others • Individuals fail to show anxiety, remorse, empaty, or guilt for their behaviors • Sometimes called ‘sociopaths’ • Truly don’t care about anyone else
Dissociative Disorders • Person experiences a sudden disruption in one’s memory, consciousness, or identity dis (un, non, opposite) associate (with, together, linked) Dissociate = not together
Dissociative Identity Disorder: Person appears to have more than one identity or personality. • Commonly called Multiple Personality Disorder • Some famous cases were fakes Dissociative Fugue: Sudden loss of personal memory and the adoption of a new identity in a new place
Schizophrenia • Schizophrenia is a pattern of extremely disturbed thinking, emotion, perception, and behavior. The mind is fragmented. • Ability to communicate and relate to others is severely impaired • word salads • Most aspects of daily functioning are disrupted
Symptoms of Schizophrenia Hallucinations: a sensory experience (seeing, hearing) when there is no basis for it. • Difficulty in focusing attention, too many stimuli coming in at once Delusions: false beliefs about reality • “I’m the king of France” “The CIA is out to get me”
Types of Schizophrenia Paranoid: believes the world is out to get them. Delusional thoughts of persecution or of a grandiose nature. Difficult to treat. Catatonic: Not responsive to the outside world. Must have set routine. Disorganized: No pattern to behavior, flat affect (no facial expression), inappropriate laughter.
Organic disturbances Organic disturbance is when psychological function is harmed by a distinct medical problem in the brain: Brain injury, head trauma, infectious disease, toxins or poisons, Alzheimer's, etc.
Treatment approaches Psychoanalytic: based on the work of Sigmund Freud, psychoanalysis sees unconscious conflicts or repressed urges as the source of disorders. Therapists use free association, dream analysis, Rorschach tests, to uncover the unconscious causes.
Treatment approaches Psychoanalytic approach Key terms in psychoanalytic therapy: Resistance: patients don’t want to go into their unconscious, they resist Transference: patients transfer the unconscious emotion onto the therapist. Examples: become hostile or fall in love.
Treatment approaches Cognitive: Seeks to change the way the patient thinks. Looks at how irrational beliefs or incorrect assumptions harm the patient. How does the patient process information or interpret the events around them? Rational-emotive therapy is a cognitive therapy that challenges the patient so they can see how their beliefs, assumptions and thinking are interfering with their life.
Behavioral: Does not worry about internal processes. Simply seeks to change the behavior. Believes that all behavior is learned patterns shaped by reinforcement and punishment. Token-economies: provide positive reinforcement for desired behaviors in the form of tokens that can be collected and used for rewards. Used with Autism and developmental disorders Extinction: ignore unwanted behavior
Humanistic: Seeks to emphasize the patients ability to grow and fulfill their potential. Led to development of group therapy where people help each other feel supported and not alone. Client-centered therapy: developed by Carl Rogers, client-centered therapy has the therapist be a cheerleader for the patient to build their self-esteem. Therapists show Unconditional Positive Regard for clients.
Medical Model (Biomedical): Disorders are thought of as physiological more than psychological. They are based on chemical imbalances, so they are treated with medication. Socio-Cultural approach: disorders come from the influence of society and are just behaviors rejected by the dominant culture.
Important Terms • Sense: A system that translates information from outside the nervous system into neural activity • Sensations: Messages from the senses • Perception: The process of making sensations into meaningful experiences
Perceptual Processing • Bottom-up processing: Aspects of recognition that depend first on the information about the stimulus that comes up to the brain from the sensory receptors
Perceptual Processing • Top-down processing: Those aspects of recognition that are guided by higher-level cognitive processes and psychological factors such as knowledge and expectations and desires
Top-Down Processing Information processing guided by higher-level mental processes as we construct perceptions, drawing on our experience and expectations. THE CHT
Priming Priming: When a prior stimulus makes the brain more ready (predisposed) to perceive or detect a certain type of future stimulus. • Example: Show students a picture of a bunny, later ask them to spell “hair” and more of them will spell it “hare”
Attention • We have lots of stimuli coming in. We can use Selective Attention to “tune in” to what we want to see or hear. But sometimes our attention controls us. (Thalamus) • Cocktail Party effect – when we hear our name, we suddenly pay attention to a conversation we were not following.
Transduction • The process of converting the physical sensation into a neural transmission. • When energy from the world (light, sound waves, heat, etc.) becomes pulses of neurons firing.
Localization of Sounds Because we have two ears, sounds that reach one ear faster than the other ear cause us to localize the sound.
Light waves and Sound waves • For waves of light the wavelength/frequency determines the color of the light. ROYGBIV • The amplitude determines the brightness or intensity of the light. • For sound, wavelength/frequency determines the pitch of the sound. High frequency = high pitches • The amplitude of the wave determines the loudness of the sound. An amp.
Parts of the eye • Cornea: Transparent tissue where light enters the eye. • Iris: Muscle that expands and contracts to change the size of the opening (pupil) for light. • Lens: Focuses the light rays on the retina. • Retina: Contains rods and cones that do Transduction of light into neurons firing to the brain.