Download
1 / 40
400 likes | 543 Vues
Improving Care in a Learning Health Care System. Richard B. Colletti , MD Vice Chair for Clinical and Research Affairs. Overview. Reliability in health care Application of the Model for Improvement to pediatric IBD ImproveCareNow

E N D
Improving Care in a Learning Health Care System Richard B. Colletti, MD Vice Chair for Clinical and Research Affairs
Overview • Reliability in health care • Application of the Model for Improvement to pediatric IBD • ImproveCareNow • Improving care and outcomes for children with Crohn’s disease and ulcerative colitis • Collaborative Chronic Care Network (C3N) • Learning Health Care System
What was the probability… • that my plane would crash?1 in 1,000,000 (failure rate)Reliability rate: 99.9999% • that my bag would not arrive?1 in 100 (failure rate)Reliability rate: 99% • that my plane would arrive late?1 in 10 or worse (failure rate)Reliability rate: 90%
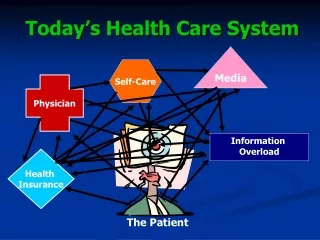
What is the reliability of medical care? • Patients receive only 60% of recommended care • Patients take only 60% of recommended medications • There is a gap between recommended care and the care actually carried out • If medical care and patient self-management were more reliable, would outcomes be better? 5
Remission rate Centers with >75% enrolled % of patients by disease status 77% 18% 5% ••Inactive•• ••Mild•• ••Moderate-Severe••
How we improve care and outcomes PracticeGuideline • Establish Aims and MeasuresWhat are we trying to accomplish? How would we know if a change is an improvement? • Measure performance • Identify gaps between standard and actual performance • Make changes to close the gaps using tools to increase reliability
14,200 IBD patients 46 centers 425 Ped GI 30%
How many patients in the registry? 8,700 enrolled A gold mine of data for learning 45,000 visits Largest and fastest growing in the world
Data collection and entry • Enroll every patient with inflammatory bowel disease • Enter data for every outpatient visit • 50 to 75 data elements each visit • Manual web-based data entry into registry
9 process measures: Classification bundle 5 classifications: disease severity, extent, phenotype; nutrition & growth
6 outcome measures: Remission rate 2007 2010 2011 2008 2009
Data entry Data collection Data storage Patient visit Plan and carry out changes Act Plan Data analysis Report analysis Study Do Reports to sites R.Colletti 2009
MONTHLY DATA QUALITY REPORT Control charts and Exceptions Report
Communicate & Collaborate 2007 R.Colletti 2004 19
Communications • Listserv • ImproveCareNow Portal (on-line resource center) • www.ImproveCareNow.org • Weekly Digest • eNewsletter: Circle • Blog: Loop • eNewsletter for practitioners: Scope • Facebook, Twitter, YouTube
Interventions • Registry enrollment and data quality • Model IBD Care guideline • Population management • Care stratification • Pre-visit planning • Self-management support
COMING SOON: AUTOMATED POPULATION MANAGEMENT & CARE STRATIFICATION
ImproveCareNow Current State: Data Recorded Three Times Encounter Data Entry Abstraction
ImproveCareNow Coming Soon:Data-in-Once, Files Uploaded Analysis QI CER Encounter
C3N ProjectCollaborative Chronic Care Networks • NIH TR01 grant • Transform ImproveCareNow into a C3N • Join patients, parents, clinicians and researchers in a shared collaborative network • Improve clinical practice, patient self-management, and disease outcomes • Innovative prototypes • YouMeIBD.com, Passive PRO app, mentoring program, N of 1 Trials with PRO app, Peer Produced Practice Knowledge, mobile social games • Patient Advisory Council, Parent Working Group, Building Community Leadership, patient platform: create a patient- and family-centered network
Learning Healthcare System “Designed to generate and apply the best evidence for the collaborative choices of each patient and provider; to drive the process of discovery as a natural outgrowth of patient care; and to ensure innovation, quality, safety, and value in health care”
Learning Health Care System • Community • Focus on the outcome • Data-in-once • Quality improvement • Comparative effectiveness • Governance
Using data for research as well as QI: Simulated trial Outcomes ImproveCareNow n=96; REACH n=112 NS NS
The value equation Value = outcomes cost
Purpose of ImproveCareNow Transformthe health, care and costs for allchildren and adolescents with Crohn’s disease and ulcerative colitis by building a sustainablecollaborative chronic care network, enabling patients, families, clinicians and researchers to work together in a learning health care system to accelerate innovation, discovery and the application of new knowledge. September 2012