The DSM-V
The DSM-V. From Malleus Malleficarum to DSM-V Diagnostic and Statistical Manual of Mental Disorders (DSM) is a system that contains the the American Psychiatric Association (APA) criteria for mental disorders . orginated in 1952, c urrently on fif th edition .

The DSM-V
E N D
Presentation Transcript
The DSM-V • From Malleus Malleficarum to DSM-V • Diagnostic and Statistical Manual of Mental Disorders (DSM) is a system that contains the the American Psychiatric Association (APA) criteria for mental disorders. • orginated in 1952, currently on fifth edition. • Has 17 different classes of disorders.
The DSM-V • Provides list of diagnostic criteria and a set of decision rules for each condition. • Warns to “think organic” (eliminate physical causes of symptoms at first). • Contains information on prevalence and assess patients along five axes. Prevalence is the percentage of people within a populationwho have a specific mental disorder.
DSM-V Axes: biopsychosocial approach • Axis I – Major mental disorders • Axis II – Personality disorders and MR • Axis III – Associated medical conditions • Axis IV – Life stressors • Axis V – Overall level of daily functioning
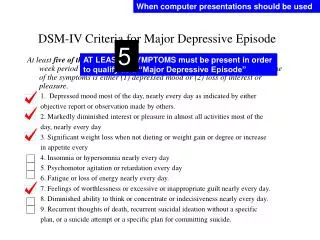
Table 15.4 (continued) The DSM-IV Criteria for Major Depressive Disorder.
DSM Criticisms • Not all diagnoses meet Robins and Guze criteria for validity (such as Mathematics Disorder). • Not all criteria are based on scientific data. Some of them are based on subjective committee decisions. • High level of comorbidity= individuals with onediagnosis frequently have one or more additional diagnoses.major depression ++ one or more anxiety disorders.
DSM Criticisms • Reliance on categorical rather than dimensional model of psychopathology. • Reluctance to change (cognitive misers). • Vulnerable to political and social influences.
NORMALITY AND ABNORMALITY:A SPECTRUM OF SEVERITY • You may wonder, “Is my behavior abnormal?” or “Maybe myproblems are more serious than I thought.” • medical students’ syndrome
Mental Illness and the Law • One of the myths isthat people with mental illness are at heightened risk for violence. In fact, the majority of people with schizophrenia are not aggressive or violent.
Emniyet Genel Müdürlüğü, şiddet eğitimli şizofreni hastalarının polis kontrolünde tutulması için çalışma başlattı • Emniyet yetkilileri, Antalya'da Ekim ayında 3 polisin öldürülmesi olayının faili Çağrı Danışman'ın şizofren olduğunun ortaya çıkması üzerine şiddet eğilimli şizofreni hastalarının polis kontrolünde tutulması için çalışma başlattı. Sağlık Bakanlığı yetkilileriyle temasa geçen EGM yetkilileri, şizofrenlerin sağlık ve adres bilgilerini alıp karakollara bildirecek. Böylece her karakol, kendi mıntıkasında kaç şizofreni hastası bulunduğunu, bu hastaların nerede, kimlerle yaşadığını ve ne iş yaptıklarını bilecek.Polis, şiddet ve cinayet eğilimli hastaların durumunu periyodik olarak takip ederek, önleyici tedbirler alacak. Tedavi gören ya da hiç hastaneye gitmemiş şizofrenlerin kayıt altına alınmasıyla şizofrenlerin suç işlemesinin engellenmesi amaçlanıyor. ŞİZOFRENİ TANILI BİREYLER ŞİDDET DAVRANIŞI GÖSTERMEYE DAHA YATKIN ???Araştırmalar Türkiye 'de şizofrenler tarafından öldürülenlerin yüzde 69,4'ünün aile içinden biri olduğunu ortaya koyuyor. Türkiye'deki cinayetlerin yaklaşık yüzde 3'ü, ABD 'de ise yüzde 5'i şizofrenler tarafından işleniyor. Şizofreni tanılı bireylerin şiddet davranışı göstermeye daha yatkın olduğunu ortaya koyan araştırmalar, cinayet işleyen şizofreni tanılı bireylerin tüm cinayet vakaları içindeki yaygınlığının, şizofreninin toplumsal yaygınlığından daha yüksek olduğunu gösteriyor.
Insanity defenseare based on the M’Naghten rule, which requires people to • 1) Not know what they were doing at time of crime. • 2) Not know what they were doing was wrong. • Less than 1% of criminal cases use this successfully.
Mental Illness and the Law • Involuntary commitment is a procedure for protecting us from certain people with mental disorders and protecting them from themselves, by placing them in a psychiatric hospital.
Anxiety Disorders • Most anxieties are transient and can be adaptive. • They canspin out of control and become excessive and inappropriate. • One of the most prevalent and earliest onset of all classes of disorders.
Many anxiety disorders, including phobias, frequently have an initial onset in childhood.
Anxiety Disorders • Can also see inappropriate anxiety in other disorders and problems. Anxiety isn’t limited to anxiety disorders. • Somatoform disorders are physical symptoms with psychological origins. • Hypochondriasis is a preoccupation that you have a serious physical disease despite no evidence.
Generalized Anxiety Disorder • Continual feelings of worry, anxiety, physical tension, and irritability about many areas. Worry is a way of life. • Many describe themselves as “worry warts.” • About 3% of the population; 1/3 develop it after major stressor or life change. • More prevalent in females and Caucasians.
Panic Disorder • Repeated, unexpected panic attacks, along with either • Persistent concerns about future attacks. • A change in personal behavior in an attempt to avoid them. • Can be associated with specific situation (such as riding in elevators or shopping in supermarkets), or come “out of the blue.”
Symptoms of a panic attack include a pounding or racing heart, shortness of breath, and faintness or dizziness. This can lead people to believe they are having a heart attack.
Phobias • Intense fear of an object or situation that’s greatly out of proportion to its actual threat. • Most common anxiety disorder (11%) • Comes in different forms • Agoraphobia. • Specific or • Social phobia.
Some of the most common fears involve insects and animals, such as spiders and snakes.
Posttraumatic Stress Disorder • Marked emotional disturbance after you experience or witness a severely stressful event, such as combat, an earthquake,or sexual assault. • The event must be physically dangerous orlife-threatening, either to oneself or other. • Symptoms include • Flashbacks and recurrent dreams. • Avoiding reminders of the trauma. • Increased physiological arousal, (sleep difficulties and startling easily).
PTSD involves a constellation of symptoms that can be quite debilitating.
Obsessive-Compulsive Disorder • Marked by obsessions - persistent ideas, thoughts, or impulses that are unwanted and inappropriate and cause marked distress. They center on “unacceptable” thoughts about such topics as contamination, sex, aggression, or religion.People with OCD are disturbed by their thoughts and see them as irrational. • This distress is relieved by compulsions – repetitive behaviors or mental actsthat they undertake to reduce or preventdistress, or relieve shame and guilt. • Must spend at least 1 hour per day engaging in obsessions, compulsions, or both.