Download
1 / 51
600 likes | 1.43k Vues
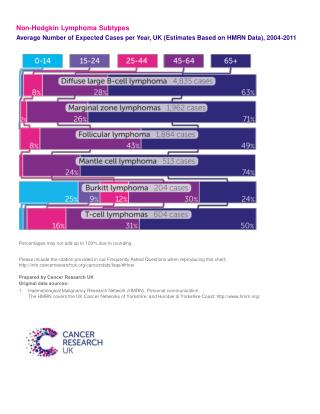
Hodgkin Lymphoma Board Review . Brad Kahl, MD 11/18/03. Hodgkin Lymphoma. Epidemiology Biology Classification Approach to the Patient. Hodgkin Lymphoma. Epidemiology 14% of malignant lymphomas 0.5% of all malignancies approximately 8000 new cases/yr in US approximately 1500 deaths/yr

E N D
Hodgkin Lymphoma Board Review Brad Kahl, MD 11/18/03
Hodgkin Lymphoma • Epidemiology • Biology • Classification • Approach to the Patient
Hodgkin Lymphoma • Epidemiology • 14% of malignant lymphomas • 0.5% of all malignancies • approximately 8000 new cases/yr in US • approximately 1500 deaths/yr • over past 30 years • age adjusted incidence rates declined appreciably • mortality rates declined substantially
Hodgkin Lymphoma • Epidemiology • men > women • whites > blacks > Asians • no clear risk factors, several implicated • woodworking, farming • familial risk • Concordance for HD in twins • 10/179 in monozygotic vs 0/187 in dizygotic twins (Mack et al, NEJM 1995)
Hodgkin Lymphoma • Risk Factors con’t • HIV • increases risk for HD 8 fold • HD not an AIDS defining illness • NHL 113x • KS 310x • Unclear why risk for NHL so much greater in HIV patients compared to HD
Hodgkin Lymphoma • Epstein Barr Virus • EBV DNA found in 50% RS cells • pathogen or passenger • Increased risk for HD after infectious mono (Hjalgrim et al, NEJM 2003) • Absolute risk 1/1000 • Median incubation time from mono to EBV+ HD 4.1 years • No increased risk for EBV- HD after mono
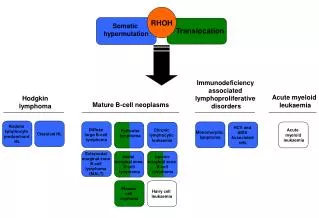
Hodgkin Biology • Hodgkin’s Disease • Reed-Sternberg cell is the malignant cell • 1% of cells in a biopsy specimen • potent cytokine producing cell (at least 12 cytokines) • cytokines appear to drive the disease process • remainder of cells are background inflammatory cells • lymphocytes, plasma cells, macrophages, eosinophils • RS cell as the malignant cell • origin only worked out within the past 5 years
Hodgkin Biology • RS is a “crippled” germinal center B cell • does not have normal B cell surface antigens • micromanipulation of single RS followed by PCR demonstrates clonally rearranged, but non functional immunoglobulin genes • somatic mutations result in stop codon (no sIg) • no apoptotic death malignant transformation • unclear how this occurs; ? EBV • unclear how cells end up with RS phenotype
Hodgkin Lymphoma Classification • “Classic” Hodgkin’s Disease • nodular sclerosis • mixed cellularity • lymphocyte depleted (very rare) • classical lymphocyte rich • HRS cells CD30 and CD15 positive • nodular lymphocyte predominant • HRS cells (L&H cells) have B cell markers • CD 20 and surface Immunoglobulin
NLP Hodgkin Lymphoma • differs from classical HD clinically and histopathlogically • preference for peripheral nodal sites • early stage distribution • late median time to recurrence • late recurrences common • low mortality from HD • L&H cells • express CD 20 (B cell marker) • express surface Ig
Nodular Lymphocyte Predominant Hodgkin Lymphoma • Management • No consensus • often treated like classical hodgkins • My view is “do not overtreat” as cure is unlikely and as many deaths from second malignancies as from LPHD (possible related to HD therapy) • I believe watch and wait is reasonable • Often can do IFRT to problem areas as they appear • Rituximab effective in relapse with ORR 85-100%.
Hodgkin Lymphoma: approach to patient • staging evaluation • H & P • CBC, diff, plts • ESR, LDH, albumin, LFT’s, Cr • CT scans chest/abd/pelvis, CXR • bone marrow evaluation (for stage IIB and higher) • PET scan may be helpful • PFTs, LVEF when clinically indicated • Fertility counseling • **lymphangiogram or laparotomy**
Modified Ann Arbor Staging Stage I Involvement of a single lymph node region Stage II Involvement of 2 lymph node regions on the same side of the diaphragm Stage III Involvement of lymph node regions on both sides of the diaphragm Stage IV Multifocal involvement of 1 extralymphatic sites ± associated lymph nodes or isolated extralymphatic organ involvement with distant nodal involvement Cancer. 1982;49:2112.
Ann Arbor Staging System for Hodgkin's Disease and Non-Hodgkin's Lymphoma Stage I Stage II Stage III Stage IV Reprinted with permission. Adapted from Skarin. Dana-Farber Cancer Institute Atlas of Diagnostic Oncology. 1991.
Modified Ann Arbor Staging • “E” designation for extranodal disease • B symptoms • recurrent drenching night sweats during previous month • unexplained, persistent, or recurrent fever with temps above 38 C during the previous month • unexplained weight loss of more than 10% of the body weight during the previous 6 months • Criteria for bulk • 10 cm nodal mass • mediastinal mass > 1/3 thorax diameter
Hodgkin Lymphoma: Prognostic Factors • Adverse prognostic features for stage I & II (EORTC data) • more than 3 nodal sites • bulky adenopathy • ESR > 50 • B symptoms • invasion into critical organs • male • age > 40 • MC or LD subtype • should probably not receive XRT alone if any of the above present (excessive relapse rate)
Hodgkin Lymphoma: Prognostic Factors • Independent adverse prognostic factors • advanced stage (III-IV) • male sex • age > 45 • albumin < 4 gm/dl • HgB < 10.5 mg/dl • stage IV disease • WBC count > 15,000/mm3 • lymphocyte count < 600/mm3 (Hasenclever et al, NEJM 339,1506-1514;1998)
Hodgkin Lymphoma: Biologic Prognostic Factors • Favorable • EBV in tumor cells • Unfavorable • Tissue eosinophila (NSHD) • Lymphocyte depletion (NSHD) • RS atypia (NSHD) • Bcl-2 overexpression • P53 • High proliferative rate
Hodgkin Lymphoma • Treatment • approach depends upon stage, prognostic factors, and co-morbidities • Stage I-II • consider XRT, chemotherapy, or combined therapy • Bulky stage I-II • combined modality therapy, usually 6 cycles of chemotherapy • Stage III-IV • ABVD x 6-8 cycles gold standard
Hodgkin Lymphoma • Results of Treatment stage5 year overall survival • I 90% • II 90% • III 80% • IV 65%
Hodgkin Lymphoma: Treatment of limited stage disease • Current general consensus is to administer CMT • ABVD x 4 (consider 6 cycles for bulk) • Followed by IFRT • Definite trend towards limiting the radiation field and possibly lowering the radiation dose due to concern over late effects • Data from 2 large trials • #1: Institute Nazionale Tumori • Enrolled patients with stage I, IIA, IIA bulky, and IIEA • Data presented at 2001 ASH meeting
Hodgkin Lymphoma: Treatment of limited stage disease • Study #2: Engart et al, JCO Oct 2003. • Included patients with limited stage HD and at least one risk factor • Bulky mediastinal disease • Extranodal disease • Massive splenic disease • ESR > 50 and no B symptoms • ESR > 30 and B symptoms • More that 2 lymph node regions
Hodgkin Lymphoma: Treatment of limited stage disease • More acute toxicities in EFRT • Late toxicities (second CA, cardiac, pulmonary) not statistically different • Trend worse in EFRT arm • Longer follow up will needed • Conclusion from trials 1 and 2 • 4 cycles of chemotherapy plus IFRT equally effective to treatment plans including larger radiation fields
Hodgkin Lymphoma • Excess death rate (relative)* (SEER data) • 2 years: 5.6% • 5 years: 8.8% • 10 years: 14.3% • 15 years: 19.4% • 20 years: 23.9% *compared to age and sex matched control (deaths other than from Hodgkins)
Hodgkin Lymphoma: Late Complications • Radiotherapy appears to confer the most late risk • Actuarial rate of second CA 1%/year with no plateau • In one study the 25 year cumulative risk of breast CA was 16.3% • Current major focus of current clinical trials to to maintain high cure rate while minimizing late complication • shorter courses of chemotherapy with lower radiation doses in smaller fields • elimination of radiotherapy (some argue for this already)
Hodgkin Lymphoma • Current EORTC trial for stage I-II patients • EBVP x 6 + 36 Gy IF • EBVP x 6 + 20 Gy IF • EBVP x 6 (arm closed do to excessive relapse) • Current GHSG trial for stage I-II patients • ABVD x 4 + 30 Gy IF • ABVD x 4 + 20 GY IF • ABVD x 2 + 30 Gy IF • ABVD x 2 + 20 GY IF
Hodgkin Lymphoma: Late Complications • Other Late Complications • depends upon treatment modality utilized • XRT vs. MOPP vs. ABVD vs. CMT • issues depends upon the age of patient • relative risks higher in younger patients • absolute risks higher in older patients • Risks of leukemia and infertility appear substantially lower using ABVD rather than MOPP • Infertility 20% vs. 50-70% • Pulmonary-Bleomycin, Cardiac-adriamycin
Hodgkin Lymphoma: Advanced Disease • More straightforward right now • ABVD is standard • Treat until CR + 2 cycles up to maximum of 8 • No role for routine XRT after chemo • (Aleman et al, NEJM June 2003) • Common practice is to administer consolidative XRT to bulky mediastinal disease after chemo • Stanford V, BEACOPP being compared to ABVD in prospective clinical trials currently
Hodgkin Lymphoma: Stem Cell Transplant • Reserved for patients who relapse after chemotherapy (autologous) • Superior to additional conventional chemotherapy in RCT • (Schmitz et al, Lancet 2002) • Upfront transplant for poor prognosis disease does not appear superior (2 trials) • Beneficial for the small group of patients with primary refractory HD
Lymphoma and Pregnancy • 4th most common malignancy among pregnant females (breast > cervical > ovarian) • no good evidence that pregnancy has a prognostic influence on the lymphoma (except Burkitts) • Staging Issues • CT scans and radioisotope scans contraindicated • rely on PE, labs, CXR, US, MRI, and marrow
Lymphoma and Pregnancy • Therapy during pregnancy • choices will vary on case by case basis • type of lymphoma, gestational age, personal beliefs • therapeutic abortion vs watchful waiting vs limited XRT vs chemotherapy • Indolent NHL (rare) and some Hodgkins • will be able to defer therapy until after delivery
Lymphoma and Pregnancy • Aggressive NHL and Hodgkins requiring therapy • 2nd and 3rd trimester • data suggests can give combination chemotherapy with minimal risk to fetus (CHOP or ABVD) • need to plan delivery to avoid neutropenia and thrombocytopenia • 1st trimester (most difficult situation) • consider therapeutic abortion • risk of fetal malformation with combination chemo approximately 20%