Peri-implantitis
Peri-implantitis. An inflammatory reaction, with the loss of supporting bone in the tissues surrounding a functioning implant . What we need to know. What Is peri-implantitis ? Clinical findings to look for Contributing factors Prevention Treatment . Peri - implantitis KRISTEN.

Peri-implantitis
E N D
Presentation Transcript
Peri-implantitis An inflammatory reaction, with the loss of supporting bone in the tissues surrounding a functioning implant .
What we need to know • What Is peri-implantitis? • Clinical findings to look for • Contributing factors • Prevention • Treatment
Peri-implantitis KRISTEN • Starts with a less threatening disease called Peri-Implant mucositis. • Peri-implantitis -described as an inflammatory, bacterial driven destruction of the implant-supporting apparatus. • Inflammation -a complex reaction of the body in response to an infectious agent, antigen challenge, or injury. • Accumulation of plaque aggravates the inflammatory reaction over time, resulting in irreversible tissue destruction. • Inflammation visible within 10 to 20 days of plaque • Even during early stages of inflammation,considerable tissue damage occurs • Site-specific infection yielding many features in common with chronic adult periodontitis
Implant anatomy KRISTEN • Composed of three parts: • Titanium implant - fuses with the jawbone • Abutment - fits over portion of the implant that protrudes from the gum line. • Crown - created by a restorative dentist and fitted onto abutment for natural appearance.
Contributing Factors • Poor oral hygiene • Teeth serve as reservoirs for pathogens • As early as 1 month after implantation, putative periodontal pathogens were detected around the implants of partially edentulous patients • History of periodontitis • Periimplantmicrobiota resembles that of adult periodontitis • Occlusal overload • Loosening of screws • Systemic influences • Diabetes (uncontrolled glucose levels) • Osteoporosis (Bisphosphonate drugs)
Contributing Factors • Smoking • Higher bleeding scores • Deeper pocket depths • More signs of inflammation • More radiographic bone loss around implants • Failure rates Smokers:11.3% Non-smokers: 4.8% • Chances of developing peri-implantitis are automatically greater if original teeth were lost because of periodontal disease, caries, or recurrent trauma.
Prevention Prevention is our main purpose as dental hygienists • Regular dental visits • Education • Plaque control procedures • Particularly around implants • Mechanical instrumentation of the affected areas possessing surgical flap access should be performed. • Routine radiographs
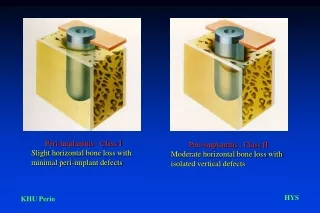
What to look for • Lack of keratinized tissue around an implant • Bleeding & suppuration upon probing • Mobility • Retention of restorations • Radiographic findings
Treatment KRISTEN • Open flap debridement • Alveolar bone and root surfaces of teeth are exposed for scaling and root planing • Implant detoxification • Calcium hydroxide and chlorhexidinegluconate may provide an antimicrobial action for detoxifying. • Calcium hydroxide should not be left in the surgical site.
A newer approach: KRISTIN • ImplanticDebrider • Water cooling agent • Cleans down between threads of visible fixture • Rotary motion - designed to remove deposits from exposed threads of affected implants • Laser therapy • Becoming increasingly common in dentistry • Applications in soft tissue surgery, caries removal, and in treatment of peri-implantitis. • Lasers irradiate the whole surface
Conclusion KRISTEN • Because dental implants are becoming more in demand, peri-implantitis is becoming more common in individuals. • Peri-implantitis is difficult to treat, therefore early detection and prevention are key. • It is crucial for patients with dental implants to have the professional care and support of a dental team. A hygienist’s goals are to encourage outstanding oral hygiene and to teach the patient which tools to use for homecare as well as to urge the patient to desire a healthy oral environment
References • Fletcher, P. (2011). Concepts for modern implantology. Dimensions of Dental Hygiene, 9(9), 44,46-48. • Heasman, P., Esmail, Z., & Barclay, C. (2010). Peri-implant disease. Dental Update, (37), 511-516. • Hempton, T. J., Bonacci, F. J., Lancaster, D., & Pechter, J. E. (2011). Implant maintenance. Dimensions of Dental Hygiene, 9(1), 58-61. • Hempton, T. J., Bonnaci, F. J., & Lassonde, M. (2011). Identifying the risks. Dimensions of Dental Hygiene, 9(5), 60-63. • Terracciano-Mortilla, L. D. (2010). Effective implant care. Dimensions of Dental Hygiene, 8(9), 30-32,34. • Petkovic-Curcin, A., Matic, S., Vojvodic, D., Stamatovic, N., & Todorovic, T., (2011). Cytokines in pathogenesis of peri-implantitis. VojnosaniteskiPregled: Military Medical & Pharmaceutical Journal of Serbia & Montenegro, 68(5), 435-440. doi:10.2298/VSP1105435P
Picture References KRISTEN • http://www.drchetan.com/dentalpics/dental-instruments/dental-implants/dental-implant-7/ • http://www.exodontia.info/files/Dental_Update_2010._Peri-Implant_Diseases.pdf