Download
1 / 24
240 likes | 583 Vues
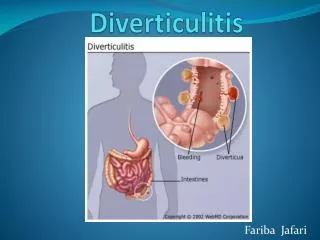
Joint Hospital Surgical Ground Round 11 th February 2012. Update on management of colonic diverticulitis. Dr. Nerissa Mak Oi Sze Department of Surgery North District Hospital/ Alice Ho Miu Ling Nethersole Hospital. Colonic Diverticulitis. A common disease 90% involving sigmoid colon

E N D
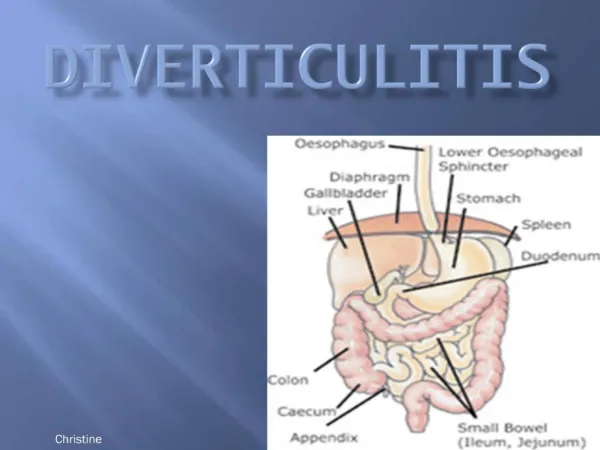
Joint Hospital Surgical Ground Round 11th February 2012 Update on management of colonic diverticulitis Dr. Nerissa Mak Oi Sze Department of Surgery North District Hospital/ Alice Ho Miu Ling Nethersole Hospital
Colonic Diverticulitis • A common disease • 90% involving sigmoid colon • Classification • Asymptomatic (diverticulosis) • Diverticulitis • Uncomplicated diverticulitis • Complicated diverticulitis • Perforation • Abscess • Fistula • Obstruction • hemorrhage Chapman et al. Ann Surg 2005
Acute management of diverticulitis Hinchey’s classification of diverticulitis & management
Evolution of management of perforated diverticulitis • 3 stage procedure • Mortality approaching 25% 1980 2000 2010 Classen et al. Ann Surg 1976
Evolution of management of perforated diverticulitis • Favor resectional surgery • Lower mortality compared with non-resectional surgery • Hartmann’s operation • Mortality drop by half compared with 3 stage procedure 1980 2000 2010 Krukowski et al. Br J Surg 1984
Evolution of management of perforated diverticulitis • Primary Resection and Anastomosis (PRA) • Comparable mortality rate with Hartmann’s operation • An effective alternative to Hartmann’s procedure 1980 2000 2010 Constantinidas et al. Dis Colon Rectum 2006
Is PRA good enough? • Mortality rate 10-20% • Morbidity rate 29% • Leakage rate 14% Any better alternatives? Salem et al. Dis Colon Rectum 2004
Evolution of management of perforated diverticulitis • Non-resectional approach: Laparoscopic Lavage • Lower morbidity & mortality • Stoma avoidance 1980 2000 2010 Mahdi Alamili et al. Dis Colon Rectum 2009
Evolution of management of perforated diverticulitis • Non-operative approach • Avoid emergent operation in >90% cases 1980 2000 2010 Sekhar Dharmarajan et al. Dis Colon Rectum 2011 Costi et al. Surg Endosc 2012
Today’s focus: For perforated diverticulitis: • Operative or non-operative approach? • Resection or non resection?
Joint Hospital Surgical Ground Round 11th February 2012 Update on management of colonic diverticulitis Management of Perforated DiverticulitisOperative Vs Non-operative
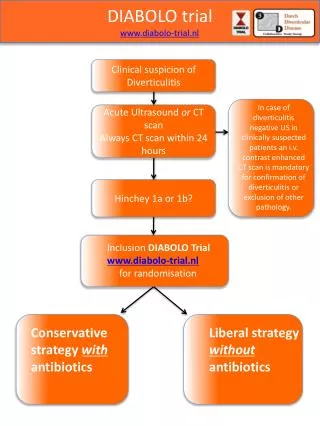
Retrospective review CT diagnosed perforated acute diverticulitis Sekhar Dharmarajan et al. Dis Colon Rectum 2011 Costi et al. Surg Endosc 2012
Contraindications of conservative management • Hemodynamically unstable • CT features suggestive of perforated communicating peritonitis • Failed rapid response to conservative management Sekhar Dharmarajan et al. Dis Colon Rectum 2011 Costi et al. Surg Endosc 2012
Conservative management in perforated diverticulitis • Pneumoperitoneum is not an indication for emergency operation • Can be attempted in case of • Hemodynamically stable • CT features not suggestive of perforated communicating peritonitis Await comparative study or multicentre prospective trials Sekhar Dharmarajan et al. Dis Colon Rectum 2011 Costi et al. Surg Endosc 2012
Joint Hospital Surgical Ground Round 11th February 2012 Update on management of colonic diverticulitis Management of Perforated Diverticulitis Resection Vs Non-Resection
Drawback of resectional approach • High mortality rate • Up to 35% after emergency operation for diverticulitis • Morbidity secondary to stoma • Up to 35-55% of patients never have the stoma reversed • Reversal of stoma also have significant morbidities McGillicuddy et al. Arch Surg 2009 Maggard et al. Am Surg 2004 Vermeulen et al. Colorectal Dis 2009
Laparoscopic Lavage in perforated diverticulitis • Low morbidity of 10% • Low mortality of 1.4% • Overall conversion rate of 3% • Shorter length of stay (median 9 days; compared with 20-38 days after Hartmann’s operation • Avoidance of colostomy Majority of patients with Hinchey Grade 3 diverticulitis can effectively be managed by laparoscopic lavage in the acute setting Mahdi Alamili et al. Dis Colon Rectum 2009
Laparoscopic LavageThe new standard of care? • The inclusion criteria was not clear • Some depends on clinical signs of peritonitis, some required surgical diagnosis of perforated diverticulitis • Relatively young age • Generally small number of patients • Lack of RCT Further evidence required to become the recommended treatment
For Hinchey Grade 4… • Only 4 studies include cases of Hinchey Grade 4 • 2 out of 8 patients failed laparoscopic treatment and required Hartmann’s procedure Larger studies are also required
In summary For perforated diverticulitis: • Non-operative management may be attempted in selected group of patients • Resection is still the standard treatment • Laparoscopic lavage is a possible alternatives