Download
1 / 22
220 likes | 375 Vues
Improving the efficiency of requesting from primary care - Conclusions from a Six Sigma Project. Dr Sharman Harris Mrs Eileen Smith, Mr Gwyn Hughes-Evans, Mrs Avril Wayte, Mr P Morris and Dr Keith Griffiths. Department of Clinical Chemistry, Ysbyty Gwynedd, Bangor, North Wales.

E N D
Improving the efficiency of requesting from primary care - Conclusions from a Six Sigma Project. Dr Sharman Harris Mrs Eileen Smith, Mr Gwyn Hughes-Evans, Mrs Avril Wayte, Mr P Morris and Dr Keith Griffiths. Department of Clinical Chemistry, Ysbyty Gwynedd, Bangor, North Wales.
Introduction • Publication of chronic disease management guidelines and targets for primary care has produced increased demand for laboratory tests - unfunded. • Demand management has an essential role in modernisation of Pathology services (Carter review, 2006). • Poor IT links (primary/secondary care) currently hinder solutions.
Background • Trust Six Sigma Management training (Consultancy). • Clinical Chemistry Six Sigma project. • Zero cost after initial Six Sigma training.
Improvement Opportunity (Business Case)Why & Why Now? • Recent internal audit - approx. 20% HbA1c tests inappropriate (clinically/GMS contract). • Inconvenience to Patients. • Demand cannot be supported with current funding. • Proposals from 2005/06 SAFF • Pathology requested to develop strategy to manage service within historic funding levels.
Project Aims • Apply Six Sigma methodology to the requesting process to reduce inappropriate requests for HbA1c. • Produce a model system for demand management of other chronic disease monitoring tests from primary care (TFT’s, lipids, U&Es [eGFR] ).
What is SIX SIGMA? • A quality management tool to improve efficiency - systematic approach. • Aims to reduce variation in a process. • Customer orientated approach - VOC, CTQ’s, SIPOC diagrams, scoping, brainstorming. • Laboratory QC processes - 6 SD ( 3SD).
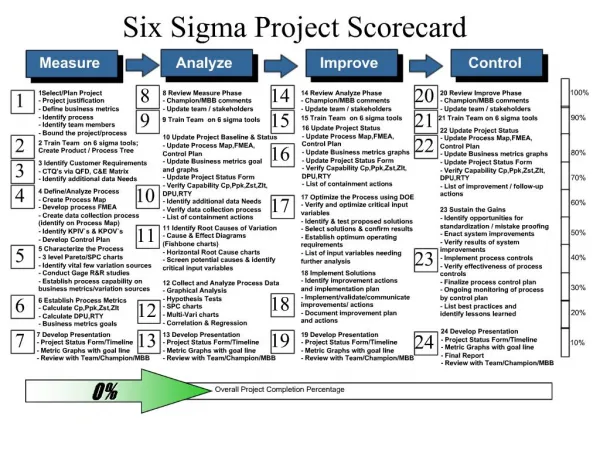
5 phases of Six Sigma Define Measure Analyse Improve Control
Project Team • Dr Keith Griffiths (Sponsor), Dr Sharman Harris (project lead), Mrs Eileen Smith, Mr Gwyn Evans, Mrs Avril Wayte (Clinical Chemistry). • Mr Peter Morris (Modernisation). • Dr Tony Wilton (Consultant Endocrinologist), Mrs Olwen Chera (ICP coordinator). • Mrs Tina Bailey (Diagnostics DGM). • LHB commissioners, Dr David Lupton (GP/LHB), Practice nurses, LHB data analysts (Karyn Donnelly, Gemma Nosworthy, Helen Adams).
Define phase • Defect definition - Stable patients (HbA1c <7.4%) having more than 2 tests/year. Based on NICE guidelines (2004) - Agreed with laboratory, Consultant endocrinologist and GP/LHB representative. • Project scoped (in frame / out of frame) In - HbA1c requests, stable patients, primary and secondary care. Out - All other tests, unstable, pregnant, newly diagnosed.
Measurement Phase • Data gather of all HbA1c results over last 24 months < 7.4%, using Telepath laboratory computer system. • Group data into patients, computer count of number of results per patient using Excel.
Baseline Sigma Value (1) • Number of units processed ie Total HbA1c results on stable diabetics (<7.4%) in 12 months • N = 10413 • Total number of defects measure I.e Inappropriate HbA1c results (> 2 results per stable patient) • D = 1038 • Number of defect opportunities per unit • 0 = 1 Look up the process sigma value in a sigma conversion table. ( 2.7)
Analysis Phase • Request process mapping. • Brainstorming-Why? change in practice, GMS contract. • Data segmentation (3 LHBs, practices). • Questionnaires (85% return rate). • Database collaboration (Trust/LHB) - number of patients and diabetics per practice etc
SIPOC/Process of HbA1c test requesting Patient appointment generated Patient attends clinic for HbA1c blood test when required and correct sample taken • All effort into increasing laboratory efficiency / reducing cost to minimum won’t cure an inefficient process. • Laboratory has opportunity to overview the process - data Test transported • Laboratory - small but central part (most of process not in department or hospital). • Laboratory affected if process inefficient via budget, (but has no control). Laboratory tests sample and returns electronic and paper report efficiently Patient attends clinic appointment where HbA1c reviewed Result acted on to benefit patient management - next appointment set.
Improvement phase • Pilot study ( 3 practices 1 from each LHB) - practice visits. • Production of a series of 1 page user guidelines (Practice nurses) - collaborative, LHB circulation. • Laboratory open evening (Practice nurses) , Practice Manager’s meetings - increase awareness. • Recalculate Interim Six Sigma value = 3.
Control phase • Weekly control Charts - circulated to LHBs at Monthly Community Pathology group meeting. • Expand Project to cover TFTs, Lipids and U&Es (eGFR).
Problems • Weekly control chart • Change Report Format ! - Number of requests generated per practice summarised as anonymous index (accounts for total number of patients and diabetics per practice). Individual practice requesting indices (forHbA1c, TFT, Lipids, U&Es) produced in a report and circulated via LHBs.
Solutions - clearer feedback • 3 month report (12 month pilot) - circulated to individual practices via LHBs. PRIMARY CARE REQUEST MONITORING REPORT You are Practice 42 (anonymous) The following practices have HbA1c requesting indices significantly higher than average. Practices 20 and 42.
Conclusions • Partnership working with budget providers and primary care. • Ongoing project (multidisciplinary). • Workload from primary care - plateau (12 month pilot).
Conclusions • Initial set up of Six Sigma project is labour intensive but template is then easily transferable. • Lessons in Communication to users - ability to adapt our approach. • IT is the ultimate aid to demand management but ………..
Thank you sharman.harris@nww-tr.nhs.wales.uk




![Six Sigma [Green Belt Project]](https://cdn5.slideserve.com/9507141/six-sigma-green-belt-project-dt.jpg)