Download
1 / 1
10 likes | 232 Vues
A study of clinical-laboratory interface involving critical laboratory values: diagnostic errors in physician ’ s interpretation of hyperkalemia Corey Chartan, MD, Satid Thammasitboon, MD, MPHE, Ayse Arikan, MD, Geeta Singhal, MD. Highly reliable decision-making system. New Reporting

E N D
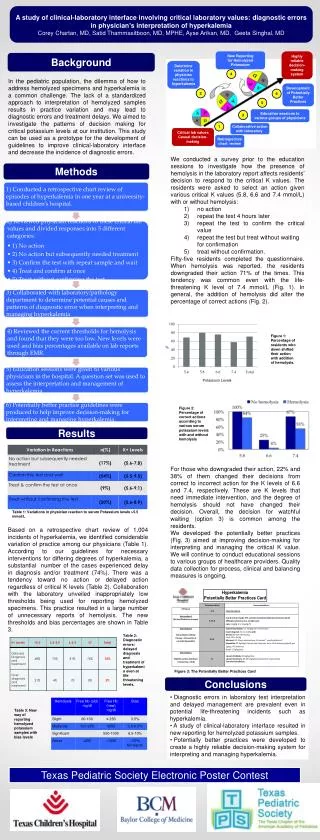
A study of clinical-laboratory interface involving critical laboratory values: diagnostic errors in physician’s interpretation of hyperkalemiaCorey Chartan, MD, Satid Thammasitboon, MD, MPHE, Ayse Arikan, MD, Geeta Singhal, MD Highly reliable decision-making system New Reporting for Hemolyzed Potassium Background Determine variation in physician reactions to hyperkalemia 4 In the pediatric population, the dilemma of how to address hemolyzed specimens and hyperkalemia is a common challenge. The lack of a standardized approach to interpretation of hemolyzed samples results in practice variation and may lead to diagnostic errors and treatment delays. We aimed to investigate the patterns of decision making for critical potassium levels at our institution. This study can be used as a prototype for the development of guidelines to improve clinical-laboratory interface and decrease the incidence of diagnostic errors. Development of Potentially Better Practices 2 6 5 Education sessions to various groups of physicians 3 1 Collaborative action with laboratory Critical lab values Casual decision-making Retrospective chart review • We conducted a survey prior to the education sessions to investigate how the presence of hemolysis in the laboratory report affects residents’ decision to respond to the critical K values. The residents were asked to select an action given various critical K values (5.8, 6.6 and 7.4 mmol/L) with or without hemolysis: • no action • repeat the test 4 hours later • repeat the test to confirm the critical value • repeat the test but treat without waiting for confirmation • treat without confirmation. • Fifty-five residents completed the questionnaire. When hemolysis was reported, the residents downgraded their action 71% of the times. This tendency was common even with the life-threatening K level of 7.4 mmol/L (Fig. 1). In general, the addition of hemolysis did alter the percentage of correct actions (Fig. 2). Methods Figure 1: Percentage of residents who down shifted their action with addition of hemolysis. % Potassium Levels Figure 2: Percentage of correct actions according to various serum potassium levels with and without hemolysis Results For those who downgraded their action, 22% and 38% of them changed their decisions from correct to incorrect action for the K levels of 6.6 and 7.4, respectively. These are K levels that need immediate intervention, and the degree of hemolysis should not have changed their decision. Overall, the decision for watchful waiting (option 3) is common among the residents. We developed the potentially better practices (Fig. 3) aimed at improving decision-making for interpreting and managing the critical K value. We will continue to conduct educational sessions to various groups of healthcare providers. Quality data collection for process, clinical and balancing measures is ongoing. Table 1: Variations in physician reaction to serum Potassium levels >5.5 mmol/L Based on a retrospective chart review of 1,004 incidents of hyperkalemia, we identified considerable variation of practice among our physicians (Table 1). According to our guidelines for necessary interventions for differing degrees of hyperkalemia, a substantial number of the cases experienced delay in diagnosis and/or treatment (74%). There was a tendency toward no action or delayed action regardless of critical K levels (Table 2). Collaboration with the laboratory unveiled inappropriately low thresholds being used for reporting hemolyzed specimens. This practice resulted in a large number of unnecessary reports of hemolysis. The new thresholds and bias percentages are shown in Table 3. Table 2: Diagnostic errors: delayed diagnosis and treatment of hyperkalemia even at life threatening levels. Figure 3: The Potentially Better Practices Card Conclusions • Diagnostic errors in laboratory test interpretation and delayed management are prevalent even in potential life-threatening incidents such as hyperkalemia. • A study of clinical-laboratory interface resulted in new reporting for hemolyzed potassium samples. • Potentially better practices were developed to create a highly reliable decision-making system for interpreting and managing hyperkalemia. Table 3: New way of reporting hemolyzed potassium samples with bias levels Texas Pediatric Society Electronic Poster Contest