Download
1 / 27
280 likes | 1.15k Vues
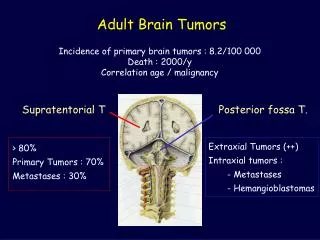
Adult Brain Tumors. Incidence of primary brain tumors : 8.2/100 000 Death : 2000/y Correlation age / malignancy. Supratentorial T. Posterior fossa T. Extraxial Tumors (++) Intraxial tumors : - Metastases - Hemangioblastomas. > 80% Primary Tumors : 70% Metastases : 30%.

E N D
Adult Brain Tumors Incidence of primary brain tumors : 8.2/100 000 Death : 2000/y Correlation age / malignancy Supratentorial T Posterior fossa T. Extraxial Tumors (++) Intraxial tumors : - Metastases - Hemangioblastomas > 80% Primary Tumors : 70% Metastases : 30%
Imaging of Brain Tumors in Adults • Who should undergo imaging ? • What is the appropriate imaging work-up ? • Differentiation from tumor-mimicking lesions • Tumor grading and extension • Optimization of treatment from imaging data
Who should undergo imaging ? • Patients at risk ? - Neurocutaneous Syndromes - Multiple sclerosis, … • Incidental Findings on MRI - Primary tumors, benign 31 (1.6) - Primary tumors, malignant 1 (<0.1) - Metastases 1 (<0.1) • Dysembryoplastic Neuroepithelial T. N Engl J Med 2007;357;18
Suggestive Symptoms of a Brain Tumor in Adults Nonmigraine, non chronic headache (70 %) Partial complex seizure (>50 %) Focal neurologic signs dependent on location (<50%) Personality changes Gait abnormalities Hemiparesia Aphasia Sensory loss Anosoagnosia Hemiparesis P F O T Visual field changes Seizure Aphasia Gait ataxia Cranial nerves palsy Pyramidal track signs
T2 T1+G FLAIR What is the Appropriate Imaging in Subjects at Risk for Brain Tumor ?
T1 (sagittal) • T1 (axial / SPGR) • FLAIR (axial) • T2* (axial) • T1 + Gd (axial) Bicommissural plane Macroscopic features Angiogenesis Detection MRI : Protocol
Detection Special case Medulloblastoma -Ependymoma Arachnoiditis Medulloblastoma
Detection Brain Metastases 1. CT • Double dose - delayed CT • Single dose and immediate CT => false negative : 11,5 %(1) 2. MRI • Gd MRI > double dose – delayed CT (2) • To increase the sensitivity • (Delayed MRI) • Magnetisation transfert • Double - Triple dose (selected cases) • Osborn. 2005 • Davis et al. AJNR 1991 • Sze G et al. AJNR 1988
0.1mmol 0.1mmol+MT T1 0.1mmol+MT 0.3mmol+MT 0.3mmol 0.3mmol+MT 0.3mmol Detection MRI : doses - MT Knauth M et al. AJNR 1996 ; 17 : 1853-9
Detection “Carcinomatous encephalitis" • Clinical signs : dementia(1) • Primitive Ca : lung, digestive tract, melanoma • Imagerie : Gd (+++), Nale(2) 1. Shirai H et al. Neuroradiology 1997 ; 39 :437-40 2. Nemzek W. AJNR 1993 ; 14 :540-2
Male, 62 y. Headache, confusion Left facial palsy Weight loss Hemorrhagic infarct ?
Infarct DWI 1H MR Spectroscopy PWI MS Tumor-Mimicking Lesions • Cerebral infarct • Radiation necrosis • Abscess • Demyelinating plaque • Subacute hematoma • Encephalitis • Post-ictal changes
Tumor vs abscess ? Low ADC = Abscess
CBV : Inflammation Tumor vs abscess ? FLAIR T1 Gd Cerebral Blood Volume
NAA = neuronal loss Lip Cho = cellular proliferation Lac Cr = hypermetabolism Lac = anaerobic metabolism Lip = necrosis 1H MR Spectroscopy Cho Cr NAA ppm 3 2 1 4
Glioma T1 Gd FLAIR Female, 20 y Partial seizure
Tumor extension Type I Type II Type III Tumoral Tissue + + - Isolated Tumor Cells - + + Spatial configuration of gliomas. C Daumas-Duport
III I II Tumor extension Pilocytic Astrocytoma Metastases Extracerebral Tumors Contrast Enhancement Tumoral Limits
III I II Tumor extension Astrocytomas, Glioblastomas Tumoral Limits : ?
III I II Tumor extension Oligodendrogliomas Low Grade Oligodendroglioma : Limits Hypersignal T2
Tumor extension Glioma vs Metastase : PWi ? Metastase : Normal perfusione Glioma : perfusion glioma Law M et al. Radiology 2002 ; 222 :715-21
Low grade astrocytoma Tumor Grading Anaplastic astrocytoma Glioblastoma
Astrocytic Tumors Assessment of the Grade 30 tumors (stereotactic biopsy) 4 senior pathologists Disagreement interobservator intraobservator Grade II A. 43 % 35 % Anaplastic A. 64 % 49 % Glioblastomas 38 % 26 % Mittler MA et al. J Neurosurg 1996;85:1091-1094
Riyadh N. et al. Intraaxial Brain Masses: MR Imaging–based Diagnostic Strategy—Initial Experience. Radiology. 2007
Localization of main white matter tracts Compression ? Infiltration ? Destruction ? ? Optimization of surgical resection Diffusion Tensor Imaging + Fiber tracking
Identification of functionnal areas : f MRI Evaluation of postoperative risks by distance tumor – functionnal area : > 2cm : no deficit 1-2cm : 33% deficit < 1 cm : 50% deficit Optimization of surgical resection lesion lesion
Prognosis of gliomas in the 1970s and today - mean time until diagnosis - time from diagnosis to treatment - perioperative morbidity and mortality rate But postoperative duration of survival has not improved Neurosurg Focus 2005