Download
1 / 50
500 likes | 646 Vues
Congressional Briefing Ethics (and Science) of Abstinence-Only Programs. John Santelli, MD, MPH Department of Population and Family Health Columbia University Tuesday, June 13, 2006 Capitol Building.

E N D
Congressional BriefingEthics (and Science) of Abstinence-Only Programs John Santelli, MD, MPH Department of Population and Family Health Columbia University Tuesday, June 13, 2006 Capitol Building
Can Changes in Sexual Behaviors among High School Students Explain the Decline in Teen Pregnancy Rates in the 1990s?Santelli, Abma, Ventura, Lindberg, Anderson, Morrow, Lyss, Hamilton Declines in pregnancy rates from 1991 to 2001 equal contributions from: • Delay in initiation of intercourse • Improvements in contraceptive use • Increased condom use • Decreased use of no method & withdrawal
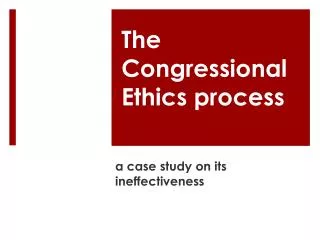
Gonorrhea — Age-specific rates among women 10-44 years of age: United States, 1981–2001
Multiple Critiques of Abstinence-Only Policies and Programs • Lack of program efficacy of AOE programs • Poorly designed, not medically accurate • “Moral” agenda not a public health agenda • Withhold vital information and promote misinformation • A cause for censorship within the public schools • Insensitive and/or unresponsive to GLBTQ and sexually active youth • Human rights and medical ethics concerns
Abstinence-Only Education:A Broader Problem? Conflicts between • Science and politics • Data and ideology
Abstinence Promotion and Abstinence-Only Policies and Programs • Epidemiology of abstinence • Initiation of sexual intercourse • Health consequences of initiating sex • Efficacy of abstinence promotion programs • Abstinence as identity movement: virginity pledges • Damage to public health program • Special issues for sexually active & GLBTQ • Human rights concerns
Public Health Value of Abstinence • Sexually active teens • Highest rates for many STIs • Highest age-specific proportion of unintended pregnancy • Initiation of sexual intercourse: • Near zero risk of deleterious health outcomes ↓↓ • State of considerable risk • Abstinence from sexual intercourse: • Healthy behavioral choice for teenagers
Changing Age at Sexual Initiation • Dramatic changes over time • Earlier age at initiation: 1960s - 1980s • Later initiation during the 1990s • High school surveys of ♂ and ♀ • Household surveys of ♂ and ♀ • Level since 2001
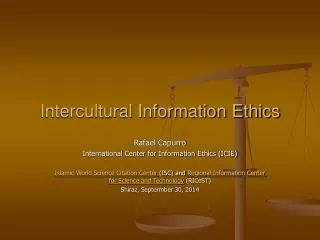
Age of First Intercourse & First Marriage in Women: 1970, 2002 First intercourse First marriage 1970 20.8 19.2 AGE 10 15 20 25 30 35 25.3 17.4 2002 First marriage First intercourse
Methodological Issues in Evaluating Abstinence Programs To demonstrate efficacy, evaluations must address: • Clear definitions of abstinence • Appropriate research design • Quasi-experimental or experimental • Measurement issues such as social desirability bias • Behavior changes as outcomes, not just attitudes • Consider biological outcomes such as STIs
Reviews of Existing Evaluations of Abstinence Education • 3 recent reviews of abstinence-only and abstinence-plus (comprehensive) programs • Kirby 2001 • Manlove 2004 • Kirby 2006 • Major national evaluation of 510 abstinence-only education currently underway
Evaluation CriteriaKirby and Manlove Reviews • Conducted since 1980 • Conducted in the United States or Canada • Targeted teens under age 18 • Experimental or quasi-experimental design • Minimum combined sample size • 100 (Kirby) • 75 (Manlove) • Generally measured sexual behavior • Kirby included studies that measured pregnancy or childbearing but not sexual behavior
Findings of New Kirby Review 6 studies of abstinence-only curricula • 0/3 delayed initiation of intercourse • 1/2 reduced multiple partners • 2/4 reduced and 1/4 increased current sexual activity 28 studies of “comprehensive” sex ed (abstinence-plus) programs • School and community-based sexuality/HIV education programs • 9 programs delayed initiation on intercourse • 18 no impact/ 1 earlier initiation
Mathematic Evaluation of Abstinence-Only Curricula Research design • Rigorous, three-part evaluation of 11 programs funded under Title V, Section 510 • Experimental design, random assignment to program or control groups • Follow up through 36 months First report (process evaluation): • Implementation, acceptance, youth development
Mathematic Evaluation of Abstinence-Only Curricula Second report (one year impact) • Increase in abstinence intentions • Small effects • Norms supportive of abstinence • Perceived consequences • No impact • Self efficacy, self esteem, perceived self control • No data on behaviors Third report (after 2005 data collection complete)
Congressional Review of Abstinence-Only Curriculum • Evidence of major errors and distortions of public health information • Eleven of 13 curricula contained false, misleading or distorted information • False information about effectiveness of contraception • Risks of abortion • Other scientific errors • Treat stereotypes as scientific fact
Studies of Abstinence Pledges(Bearman et al; Bruckner, Bearman et al) • Pledgers delay initiation of intercourse • Average delay 18 months • 88% had sex before marriage • When pledgers do initiate sexual intercourse, less likely to use condoms and contraception • Six year follow up: prevalence of STIs similar among pledgers and non-pledgers • Fewer partners but less likely to seek STI services • Oral and anal intercourse among pledgers who remain virgins
Calculating Efficacy of Abstinence • No efficacy trials of abstinence comparable to contraceptive efficacy trials • Perfect use effectiveness = 100% • Typical use effectiveness closer to 0%? • Evaluation of AOE programs • Research on virginity pledge movement
Erosion of Comprehensive Sexuality Education Abstinence-only education is replacing more comprehensive forms of sexuality education • Texas Board of Education 2003 decision: remove most information about contraception from new textbooks • Declines in teaching of comprehensive sexuality education as reported by teachers, superintendents, and young people
Erosion of Comprehensive Sexuality Education • AGI: sharp declines (1988 and 1999) in % of teachers who support teaching and who actually taught about • Birth control, abortion, and sexual orientation • School Health Policies and Programs Study (2002), School superintendents report: • 92% of middle schools and 96% of high schools taught abstinence as the best way to avoid pregnancy, HIV, and STDs • 21% of middle schools and 55% of high schools taught correct use of condoms
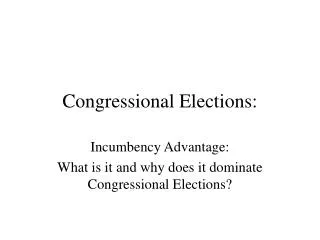
Percent of Females Ages 15-19 Ever Receiving Sex Education by Topic, 1995 and 2002
ABC Message for Title X Providers Federal guidance to Title X providers: • Education regarding the prevention of HIV/AIDS should incorporate the ’ABC‘ message. • For adolescents and unmarried individuals, the message is “A” for abstinence • For married or individuals in committed relationships, the message is “B” for being faithful • For individuals who engage in behavior that puts them at risk for HIV, the message is “C” for condom use”
Language Stressing Abstinence in CDC Content Guidelines CDC’s Interim HIV Content Guidelines for AIDS-Related Materials require that: “all programs of education and information receiving funds under this title shall include information about the harmful effects of promiscuous sexual activity and intravenous drug use, and the benefits of abstaining from such activities”
Causality of the Debate over Abstinence? Vaccines to prevent HPV/ cervical cancer • 2 vaccines nearing FDA approval • Mixed reaction among conservatives who have opposed condoms as HPV can be transmitted by skin to skin contact Bridget Maher of the Family Research Council • “Giving the HPV vaccine to young women could be potentially harmful, because they may see it as a license to engage in premarital sex”
Reproductive Rights as Human Rights • Access to accurate health information as a basic human right (Coliver and Freedman 1995) • Patients have rights to accurate and complete information from their health care providers • Withholding information or supplying misinformation to induce specific behaviors or choices by patients is inherently coercive
Ethical Obligations of Governments • Governments obligated to provided accurate information to their citizens and eschew the provision of misinformation • Provision of reproductive health care without full and impartial information leaves one vulnerable to government manipulation • International treaties and statements on human rights reinforce these obligations
Ethical Obligations of Governments U.N. Committee on the Rights of the Child (Convention on the Rights of the Child) Effective HIV/AIDS prevention requires States to refrain from censoring, withholding or intentionally misrepresenting health-related information, including sexual education and information, and that consistent with their obligations to ensure the survival, life and development of the child (Article 6), States parties must ensure children have the ability to acquire the knowledge and skills to protect themselvesand others as they begin to express their sexuality.
Ethical Obligations of Public Health Professionals • Obligation of public health professionals to provide non-judgment information about alternatives and risks and benefits of each • Ethical treatment extends to children and adolescent • A clinical example
Sexually Active and GLBTQ Youth Abstinence until marriage programs unlikely to meet health needs of sexually active or GLBTQ youth • Ignores specific needs: counseling, STI screening • Largely ignore issues surrounding homosexuality (except when discussing transmission of HIV/AIDS) • May stigmatize homosexuality and reinforce homophobia and exacerbate feelings of isolation
Insensitive to GLBTQ Youth New CBAE funding language: “Abstinence means voluntarily choosing not to engage in sexual activity until marriage.” Marriage must be defined as "only a legal union between one man and one woman as a husband and wife”
The Big Myths Scientific research does not support fears that: • Sex education and access to contraception cause teenagers to have sex • Teaching about abstinence and protection is a mixed message • Describing the limitations of contraceptive methods will stop teenagers from having sex
Conclusions • A strong case for abstinence as a short-term public health goal However • “Efficacy” of abstinence-only approaches is questionable • “Vows of abstinence break more easily than condoms” • Current federal policy: little basis in science, reflects moral opinions of the Congress • Abstinence as government policy • Eroding sexuality education, other public health efforts • Serious human rights issues • Current federal funding requirements (Subsections A-H) of Section 510 should be repealed and funding shifted to comprehensive, medically-accurate sexuality education
Federal Support for Abstinence-Only Programs • Major expansions in federal support since 1996 • Section 510 of the Social Security Act • Part of welfare reform in 1996 • support to states • Community-Based Abstinence Education projects (CBAE or SPRANS) program in 2000 • Section 510: “exclusive purpose” the promotion of abstinence outside of marriage
CBAE • 510 • AFL
Section 510 Definition of Abstinence-only Education 8 point definition: • exclusive purpose: teaching the social, psychological, and health gains to be realized by abstaining from sexual activity • teaches abstinence from sexual activity outside marriage as the expected standard for all school age children • abstinence from sexual activity is the only certain way to avoid out-of-wedlock pregnancy, sexually transmitted diseases, and other associated health problems • mutually faithful monogamous relationship in the context of marriage is the expected standardof human sexual activity
Section 510 Definition of Abstinence-only Education 8 point definition: • sexual activity outside of the context of marriage is likely to have harmful psychological and physical effects • teaches that bearing children out-of-wedlock is likely to have harmful consequences for the child, the child's parents, and society • teaches young people how to reject sexual advances and how alcohol and drug use increases vulnerability to sexual advances • teaches the importance of attaining self-sufficiency before engaging in sexual activity
FY 2006 CBAE Funding Requirements Restrict: “Sex education programs that promote the use of contraceptives are not eligible for funding under this announcement.” Define: Marriage must be defined as "only a legal union between one man and one woman as a husband and wife” ACF weblink: http://www.acf.hhs.gov/grants/open/HHS-2006-ACF-ACYF-AE-0099.html
FY 2006 CBAE Funding Requirements Assert: “Teen sexual abstinence improves preparation for stable marriage.” Require: “Teaches the potential psychological effects (e.g., depression and suicide) associated with adolescent sexual activity.” Must teach: “that teens who are sexually active are also more likely to engage in other risk behaviors such as: smoking, alcohol abuse, drug abuse, violence, and crime.”