
Epstein-Barr Virus
Epstein-Barr Virus. Juan Flores Jasmine Ibarra. Epstein-Barr Virus: Herpesviridae. dsDNA virus Enveloped Large, icosahedral. Classification: Group I. Structure. Viral proteins produced during productive infection are Early antigen (EA) Viral capsid antigen (VCA)

Epstein-Barr Virus
E N D
Presentation Transcript
Epstein-Barr Virus Juan Flores Jasmine Ibarra
Epstein-Barr Virus: Herpesviridae • dsDNA virus • Enveloped • Large, icosahedral
Structure • Viral proteins produced during productive infection are • Early antigen (EA) • Viral capsid antigen (VCA) • Glycoproteins of the membrane antigen (MA) • Structure and regulation similar to HSV infection. • Efficiency of the process is slower and time for replication is longer. • Virus interferes with induction of apoptosis in B lymphocytes • Primary infection of B lymphocytes often lead to establishment of latent infection.
Transmission • Saliva • Close oral contact • Sharing of toothbrush
Epstein-Barr Virus Case Study • A 17-year-old high school student has had low-grade fever and malaise for several days, followed by sore throat, swollen cervical lymph nodes, and increasing fatigue. The patient also notes some discomfort in the left upper quadrant of the abdomen. The sore throat, lymphadenopathy, and fever gradually resolve over the next 2 weeks, but the patient’s full energy level does not return for another 6 weeks.
1. What lab tests would confirm the diagnosis of EBV-induced mononucleosis and distinguish it from CMV infection? • The clinical diagnosis of infectious mononucleosisis suggested on the basis of the symptoms of fever, sore throat, swollen lymph glands, and the age of the patient. • Heterophileantibody test (“Monospot” test) • Rapid test for mononucleosis due to EBV • Sensitive for heterophile antibodies produced by the immune system in response to infection.
1. What lab tests would confirm the diagnosis of EBV-induced mononucleosis and distinguish it from CMV infection? • White blood cell count • 40%-70% of patients have elevated White Blood Cell (WBC) count of 10,000-20,000 cells/mL • 10% of patients have a WBC count greater than 25,000 cells/mL of blood by the second week of illness. • Approximately 80-90% of patients have lymphocytosis with more than 50% lymphocytes. 20%-40% of the lymphocytes in patients are atypical. • WBC appear larger, have a lower nuclear-to-cytoplasmic ratio, and have a nucleus that is less dense than that of normal lymphocytes.
1. What lab tests would confirm the diagnosis of EBV-induced mononucleosis and distinguish it from CMV infection? • EBV serology antigens would confirm for EBV • Viral capsid antigens • Early antigens • EBV nuclear antigen (EBNA) • Differentiation if the immunoglobulin G and M of the capsid
2. To what characteristic diagnostic feature of the disease does mononucleosis refer? • Mononucleosis • Results of antigen-independent proliferation of infected B cells that crowd out RBC and cause anemia. • Results from the expansion in numbers of T cells upon stimulation by the EBV-infected B cells. • Mononuclear cells are large, with ragged edges and have an abundance of cytoplasm. • Mononucleosis-like syndromes accompany other infections of lymphocytes including CMV and HIV. The excess of atypical lymphocytes present in the patients’ blood smear is indicative of mononucleosis.
3. What causes the swollen glands and fatigue? • Swollen glands and fatigue are caused by activation of the immune response • Long term recovery of the body from mono. • Swollen glands • Increased number of antibodies produced from the lymphocytes and the proliferation of T cells • Fatigue • Spleen inflammation • Absorbs RBC from the blood in large quantities
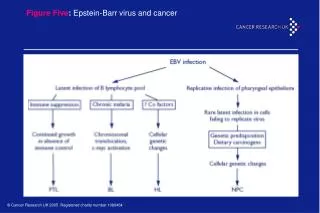
4. Who is at greatest risk for a serious outcome of an EBV infection? What is the outcome? Why? • Children • Asymptomatic disease or mild symptoms due to their less active immune system • Adolescents & adults • At risk for infectious mononucleosis • Immunocompromised individuals • At highest risk for life-threatening neoplastic disease
References • Bennett N. “Pediatric mononucleosis and Epstein-Barr Virus Infection” Medscape. (2012) Retrieved November 2012. • Murray, P.R. et al. (2005). Medical Microbiology 5th edition. Philadelphia, PA: Elsevier-Mosby • Wagner, E.K. et al. (2006). Basic Virology (3rd ed.). Malden, MA: Blackwell
![Epstein Barr Virus [EBV] - Named after Epstein and Barr](https://cdn5.slideserve.com/9727845/epstein-barr-virus-ebv-named-after-epstein-dt.jpg)
